ZYGOMATIC GLAND
The ventral buccal glands comprise a few small, solitary units located in the submucosa, rostral to the masseter muscle, medial to the ventral part of the buccinator and lateral to the mandible.
The dorsal buccal glands are consolidated in a mass generally known as the zygomatic gland (see Figures 11-10, A, 11-27Z2may stimulate respiration.
The oropharynx is dorsoventrally flattened; it extends from the palatoglossal arches, which are not easily detected unless made to stand out by pulling the tongue forward. During normal breathing the soft palate lies on the tongue with it free edge rostral to the epiglottis (Figures 11-29 and 11-33). In many brachycephalic dogs the soft palate is disproportionally long and rests over the entrance to the larynx, causing respiratory difficulties. The overlong soft palate can be shortened using the palatine vessels laterally and the palatines muscle toward the midline, as landmarks. Additional guidance is provided by the wrinkling of the palatine mucosa where it does not lie over muscle. For different
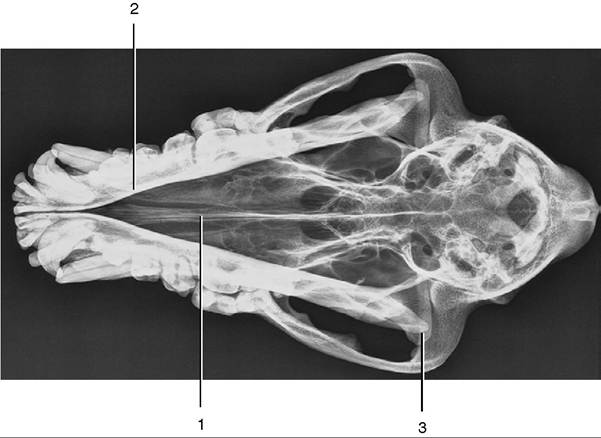
Figure 11-28 Ventrodorsal radiograph of the canine head. Note the position and size of the brain case. 1, Nasal septum; 2, mandible; 3, temporomandibular joint.
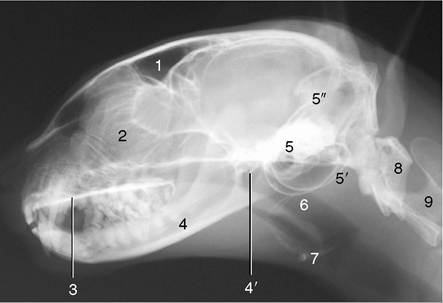
Figure 11-29 Radiograph of the feline head. 1, Frontal sinus; 2, cribriform plate and ethmoidal conchae; 3, hard palate; 4, mandible; 4', temporomandibular joint; 5, petrous temporal bone; 5, tympanic bullae; 5", tentorium cerebelli; 6, nasopharynx; 7, basihyoid; 8, atlas; 9, axis.
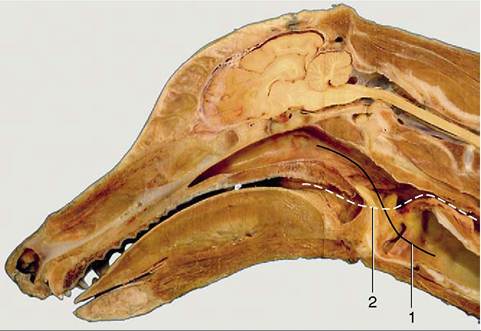
Figure 11-30 Median section of head and neck. 1, Route from nasopharynx to trachea (solid line); 2, route of food from mouth to esophagus (broken line).
reasons, the epihyoid provides a useful landmark where it crosses the lateral wall of the oropharynx. Contact with the oropharyngeal wall during examination of the mouth normally causes dogs to retch; the absence of this (gag) reflex suggests damage to the glossopharyngeal and vagal nerves.
Oral breathing is possible with the palate in the normal position (Figure 11-30), and the panting dog is a familiar sight. Cats may also breathe through the mouth but more discretely, sitting quietly and letting the air slip in and out through lips slightly parted toward the commissure. Occasionally the mouth is opened more widely, allowing a brief glimpse of the tongue.
The fusiform palatine tonsils occupy fossae in the lateral walls of the oropharynx caudal to the palatoglossal arch and ventral to the soft palate and are covered medially by semilunar folds, which arise from the ventrolateral part of the soft palate (Figures 11-17Zor breathes through the mouth, the free border of the soft palate is lodged below the epiglottis, which aligns the laryngeal lumen with that of the nasopharynx (see Figure 11-33).
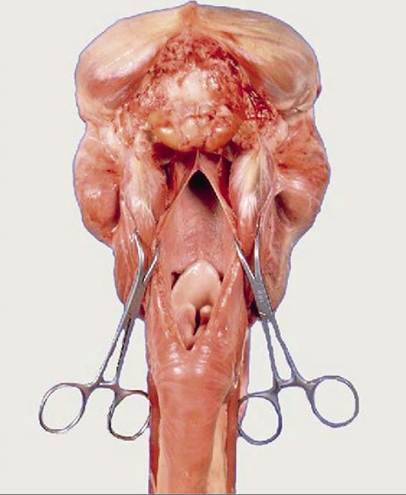
Figure 11-33 The nasopharyngeal cavity exposed by median incision of the roof. Note the postvelar position of the tip of the epiglottis.
The larynx is covered ventrally by the subcutaneous sternohyoid muscles (see Figure 11-45). It is related laterally to the medial retropharyngeal lymph node, the common carotid artery and vagosympathetic trunk, linguofacial vein, and mandibular lymph nodes. It is related dorsally to the caudal part of the laryngophar- ynx leading to the esophagus.
The sensory nerve supply to the laryngeal mucosa is from the cranial laryngeal nerve, entering the laryngeal cavity through the rostral thyroid notch. The recurrent laryngeal nerves that supply the remainder of the intrinsic laryngeal musculature, except for the cricothyroids (supplied by a branch of the cranial laryngeal nerve), leave the parent vagal trunks within the chest.
The right one arises level with the middle cervical ganglion and winds dorsally around the subclavian artery to proceed cranially in the angle between the longus colli muscle and the trachea. The left one leaves the vagus level of the aortic arch, which it loops around, distal to the ligamentum arteriosum. It ascends the neck ventromedial to the esophagus. Both nerves supply the trachea and esophagus before termination at the larynx.Laryngeal paralysis as a genetic disorder occurs in certain breeds, notably the Bouvier and Leonberger, but it has also been encountered as an occasional disorder of older dogs of other large breeds.
The cranial laryngeal arteries provide the principal blood supply. They originate from the external carotid
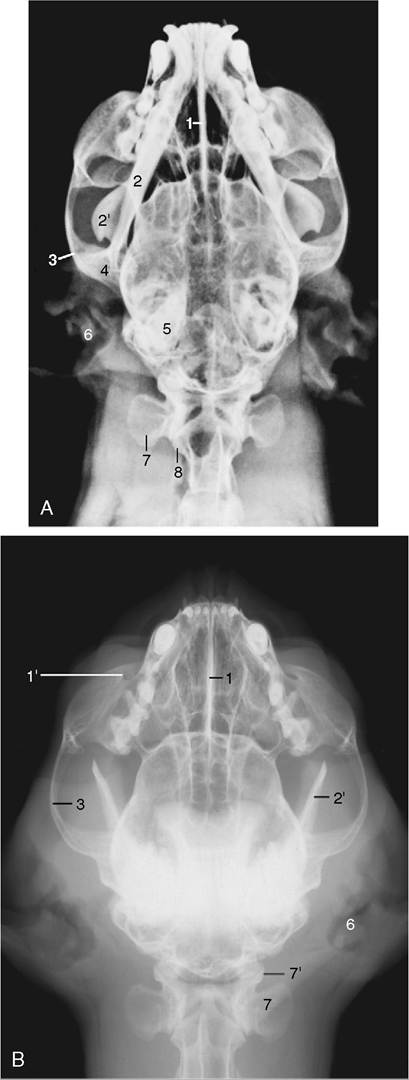
Figure 11-34 Radiographs of the feline head. A, Ventrodorsal view. B, Ventrodorsal view with mouth fully opened. 1, Nasal septum; 1', infraorbital foramen; 2, mandible; 2', coronoid process; 3, zygomatic arch; 4, temporomandibular joint; 5, petrous temporal bone; 6, external ear; 7, wing of atlas; 7', atlantooccipital joint; 8, axis.
arteries and, with the cranial laryngeal nerves, pass through the rostral thyroid notches. Satellite veins drain into the external maxillary veins. Lymphatics drain into the medial retropharyngeal lymph nodes.
The cat’s larynx is depicted in radiographs (see Figure 11-29) and in a median section (see Figure 11-35). The arytenoid cartilages have a simpler shape than those in the dog. The aryepiglottic folds bypass the arytenoid cartilages and connect the sides of the epiglottis directly to the cricoid cartilage. The vocal cords are thick and round; in contrast, the vestibular folds are thin and sharp-edged. There is no genuine ventricle, but small pouches of the vestibular mucosa extend lateral to the fold. Solitary lymph nodules are present on the laryngeal surface of the epiglottis, while aggregated nodules (paraepiglottic tonsils) thicken the aryepiglottic folds.
Electromyographic studies show that purring in cats is produced by fast twitching of muscles in the larynx and diaphragm. The laryngeal muscles rapidly narrow and widen the glottis, which causes respiratory air to vibrate and make the sound.
Differences between the upper airways of brachycephalic and mesaticephalic breeds have been mentioned from time to time. In certain breeds, the specific proportionalities in the upper airways have an adverse influence on respiratory function resulting in the brachycephalic obstruction syndrome. In this syndrome, the nostrils can be stenotic, the pharynx short and narrow with thickened redundant mucosa, the root of the tongue massive, and the soft palate overlong. The progressive dyspnea is caused by increasing body weight, relatively insufficient growth of the laryngeal structures, increasing mass of the pharyngeal mucosa, and insufficient opening of the glottis. In addition, there is progressive collapse of the laryngeal structures and eversion of the laryngeal ventricles because of the increased traction caused by the increased velocity of exhaled air passing the relatively small laryngeal opening.