Bone Marrow Collection
Sites
Hematopoietically active bone marrow is most consistently found in the flat bones (sternum, ribs, pelvis, vertebrae) and proximal ends of long bones (humerus, femur). The most
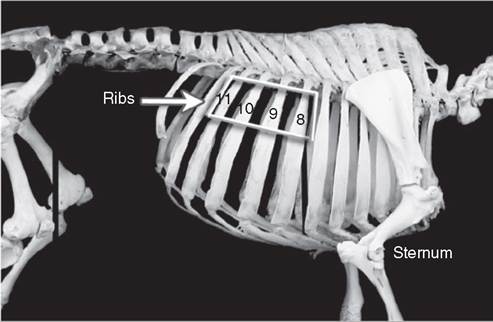
FIG.
28.2 Bovine skeleton depicting sites for bone marrow aspiration: the sternum and vertebral ends of ribs 8 to 11.commonly described sites for bone marrow aspiration in large animals are the sternum, ribs, and iliac crest (Figs. 28.1 and 28.2). Which location is chosen may depend on species, age, and temperament of the animal as well as on available facilities.
The ventral sternum is the preferred site in adult horses, small ruminants, and camelids (Figs. 28.3 to 28.6). It is one of the preferred sites in cattle. The advantages of the sternum are that it is covered by only a thin layer of bone, it has areas not covered by thick muscles, and samples can be reliably obtained from the site. The disadvantages of the sternum are that it is near vital organs and that the operator is in an awkward position when working on a standing animal. A procedure for sampling the cranial aspect of the sternum has also been described in horses10 (see Fig. 28.3). There is more muscle to go through with this approach.
The ribs are one of the preferred sites for bone marrow aspirates in cattle. The dorsal ends of ribs 8 to 11 can be accessed for sequential aspirations11 (see Fig. 28.2). Ribs can also be used in the horse, but the needle slips off the bone more easily. In calves, sheep, and goats the marrow cavity of the rib is small and more difficult to hit,12 and in camelids the rib marrow is less consistent in location than the sternum.13 Successful collection from ribs has been described in camels, with the fifth to eighth ribs as the best sites.14
The iliac crest is the site often used for bone marrow sampling in foals, and it can also be used in young adult horses up to a couple of years in age15 (Fig.
28.7). Samples can also be obtained from older horses at this site, but the needle must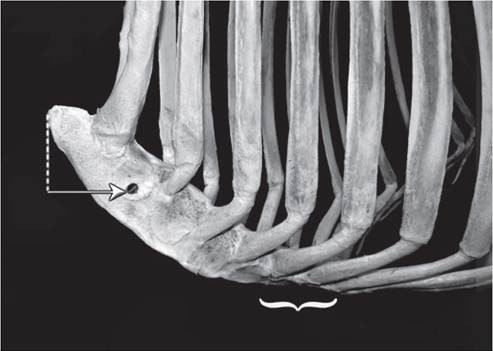
FIG. 28.3 Lateral view of equine sternum. The ventral sternum is the most popular site for sampling bone marrow in the adult horse (bracket), but the cranial sternum can also be used. The aspirate site of the cranial sternum is reached by going one hand width below (dotted line) and one hand width lateral to its cranial tip. From there, the needle is advanced in a horizontal plane at a 45-degree angle to the longitudinal axis of the horse (arrow).

FIG. 28.6 Llama sternum. The llama sternum can be sampled at ventral midline, inserting the needle vertically through the callosity, or from a lateral approach, inserting the needle dorsal to the callosity.
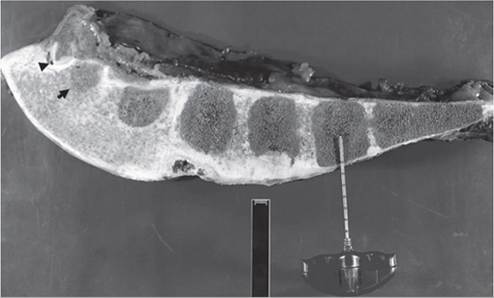
FIG. 28.4 Equine sternum sectioned on midline. The bone marrow aspiration needle is anchored in the center of the fifth sternebra. The arrowhead indicates the first sternocostal joint; left and right joints are usually fused together in horses. The black arrow indicates the first sternebra.
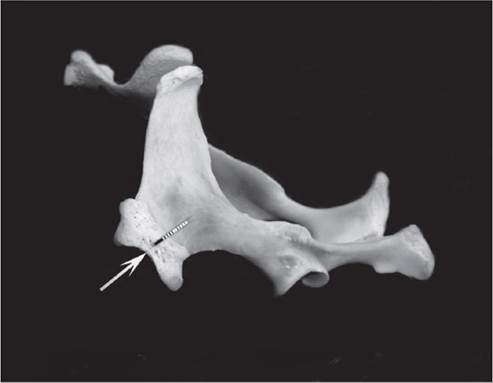
FIG. 28.7 Equine pelvis. To obtain bone marrow, the needle should be placed near the center of the tuber coxae (arrow) and advanced toward the opposite coxofemoral joint (dotted line).

FIG. 28.5 Cross-section of sheep sternum. The needle is entering the second sternebra. The second through fourth sternebrae are recommended as optimal sites for bone marrow collection.
be inserted more deeply, needle placement is more critical, and it becomes difficult to obtain a successful sample in horses more than 9 years old.16 The wing of the ilium is generally considered too thin for bone marrow aspiration in camelids,13 although successful bone marrow aspiration from the iliac crest of a 2-year-old alpaca has been reported17 (Fig.
28.8). The iliac crest can also be used in sheep (Fig. 28.9).Another site informally described for horses is the spinal process of the first lumbar vertebra (Fig. 28.10). It is usually vertical, whereas the adjacent processes tend to be more angled. The tip of the process is wider than the shaft and has a thin layer of bone. The needle is advanced straight down into the marrow cavity, which is narrow, but if the needle is close to correct placement the walls of the process help guide the needle into the marrow cavity. The advantage of this site is that the operator is not working under the horse. The spinal process is reported to be a poor site to sample in the cow.18
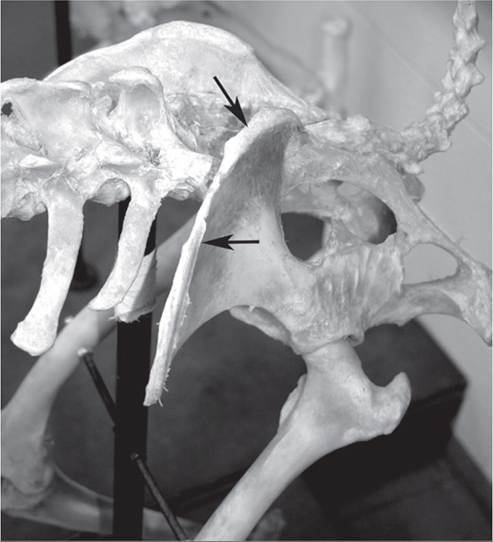
FIG. 28.8 Llama pelvis. The wing of the ilium (arrows) is generally considered too thin for easy bone marrow collection in camelids.

FIG. 28.9 Bone marrow aspirate from the ileum of a sheep. This sheep was undergoing necropsy, and the wing of the ileum has been dissected out.
Preferred collection sites to obtain equine bone marrow for regenerative therapeutic purposes include the sternum and tuber coxae. For young horses either site can be elected. However, in older animals aspirates from the tuber coxae yield significantly lower numbers of BMSCs.19 Complication rates associated with the procedure are generally low for both sites20; nevertheless, severe complications have been reported following sternal aspirates.21 In vitro, BMSCs from ileal aspirates showed higher chondrogenesis properties (glycosaminoglycan accumulation) than cells isolated from the sternum22; however, in vivo studies to validate this potential advantage are lacking.
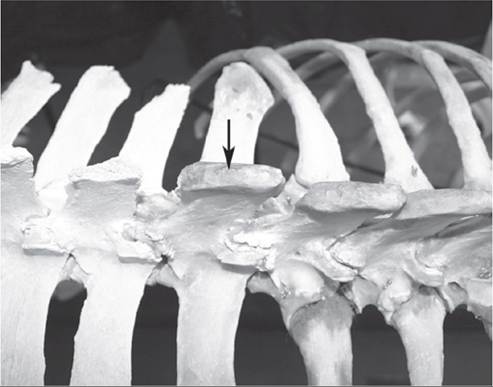
FIG. 28.10 First lumbar vertebra of a horse. Although not widely used, the spinal process of L1 (arrow) is another site from which bone marrow can be obtained in the horse.
APPROACH TO THE STERNUM. In the horse, bone marrow aspiration is typically performed in the standing animal. Sedation or a twitch may be used if necessary. The preferred site is on the ventral midline. A recent study performed in horses revealed that the fifth sternebra is the most consistent and safe site for aspiration of bone marrow.23 Ultrasound can be used to select the desired sternebra and provide guidance for the optimal puncture site (Fig. 28.11). If ultrasound is not available, the optimal insertion site is exactly on the ventral midline in the cleavage between the deep pectoral muscles where a line connecting the points of the elbows would cross24 (Fig. 28.12).
The manubrium of the sternum can also be sampled in horses by finding the cranial end of the sternum and going one hand width below and one hand width laterally from the end (see Fig. 28.3). From this spot the needle is advanced through the muscle in a horizontal plane at a 45-degree angle to the longitudinal axis of the horse.10
Sternal bone marrow can be sampled from adult cattle standing in stocks or a squeeze chute. It may be necessary to use techniques to prevent kicking, such as jacking the tail, or sedation. Unruly adult cattle and large calves can be cast and held in lateral recumbency. The upper front leg of the cast animal is held extended along the neck, exposing the sternum, after the other legs are secured with a rope.25 Calves that weigh less than 300 lb can be placed in dorsal recumbency and secured by assistants or with ropes.12 The needle should be placed on the midline and inserted perpendicular to the third or fourth sternebra. The appropriate sternebra is located by palpating the third or fourth rib and following it to the sternum.
For the sternum of a small ruminant to be sampled, the animal is placed in dorsal recumbency with legs secured, or it can be restrained in a sitting position with an assistant standing behind, supporting the animal and holding a foreleg in each hand.12 The location of the appropriate site is midline, between the front legs.
The second through fourth sternebrae can be used in sheep (see Fig. 28.5). A prominence may be felt between the first and second sternebrae. The appropriate sternebrae can also be located by palpating ribs and following them to their articulations.26 In sheep, the needle will advance approximately 0.5 cm into the bone (2.5 to 3.8 cm from the skin) before entering the marrow cavity.26The sternum of llamas can be sampled with the animal either standing in a chute or in left lateral recumbency, usually sedated27 (see Fig. 28.6). The sample can be taken by inserting
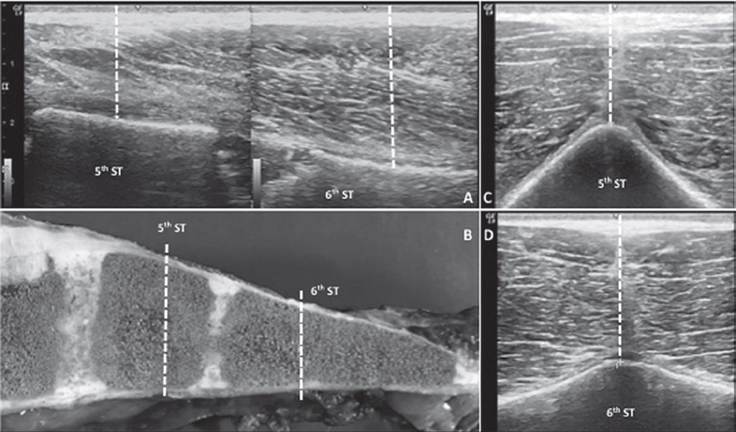
FIG. 28.11 Equine sternum. A, Longitudinal ultrasound of the fifth and sixth sternebrae. Cranial is to the left and ventral to the top of the image. The fifth sternebra is more superficial (dotted line, 1.88 cm) than the sixth sternebra (dotted line, 2.71 cm). B, Longitudinal section of equine sternum with the same orientation as in A. The fifth sternebra is more cuboidal and shorter longitudinally than the sixth sternebra. White dotted lines correspond to the position of the measuring lines in image A. Transverse ultrasound of the fifth (C) and sixth (D) sternebrae: the more conical shape of the fifth sternebra compared to the flat shape of the sixth sternebra might make it more difficult to anchor the aspiration needle in the center.
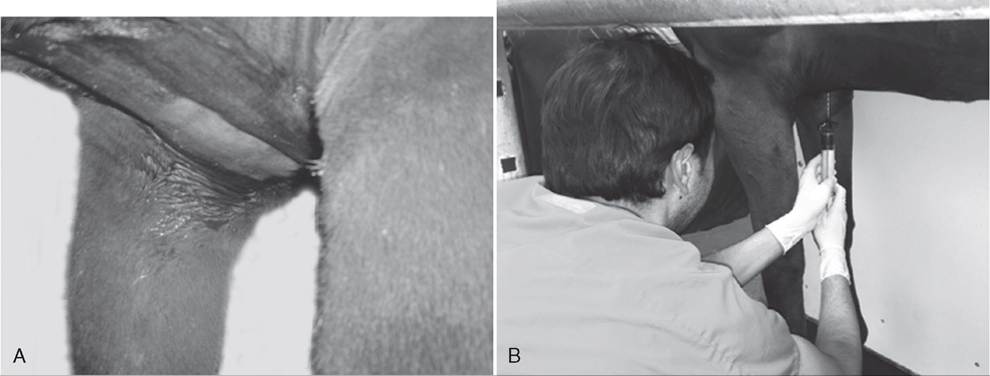
FIG. 28.12 Bone marrow aspiration in a standing, sedated horse. A, The ventral sternum between the horse’s elbows is clipped and surgically scrubbed. B, After local anesthetic and stab incision, a spinal needle is inserted at the intersection of the ventral midline with a parallel line between the points of both elbows. A heparin-primed 60-mL syringe is used for therapeutic bone marrow collection.
the needle vertically through the callosity on the ventrum of the sternum or with a lateral approach, approximately 3 to 4 cm dorsal to the callosity with the needle directed medially and slightly dorsally to engage bone.13 Marrow will be approximately 2.5 cm deep in an adult.
The sample is normally more dilute with blood than in other species.13When the ventral sternum is sampled, unless a lateral approach is used, the needle should be placed on the midline, as near to the center of the bone as possible, and advanced perpendicular to the bone. A sudden reduction of resistance may be felt when the marrow cavity is entered; because the sternal cortex is so thin, especially in horses; however, there may be no obvious change. Care needs to be taken to not enter the thoracic cavity. Because a change in resistance may not be felt, once the tip of the needle is firmly seated in the bone an aspiration attempt should be made.
APPROACH TO THE RIB. The vertebral end of the rib more consistently contains marrow than does the sternal end of the bone28,29 (Fig. 28.13). Palpation can be used to find the rib that has the least amount of fascia covering it. In the horse, the eighth to eighteenth ribs can be used, going as high as possible but below the latissimus dorsi and serratus posticus muscles28 (see Fig. 28.1). In cattle, place the needle approximately 3 inches ventral to the ninth or tenth costovertebral junction18 (Figs. 28.2 and 28.14). The needle should be inserted perpendicularly at the middle of the rib, midway between the anterior and posterior borders (see Fig. 28.14, A). To help keep the needle from sliding off the bone, a scalpel can be first inserted until it touches the bone to be used as a guide.15
APPROACH TO THE ILIAC CREST. The iliac crest is often used in foals (see Fig. 28.7). The needle should be placed
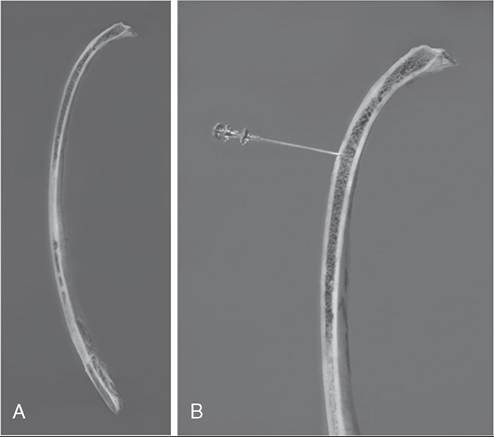
FIG. 28.13 Cross-section of bovine rib 10. A, Bone marrow is more consistently present in the vertebral end. B, Rosenthal bone marrow needle is inserted into the rib approximately 3 inches below the costovertebral junction.
■ BOX 28.2
Supply Checklist for Bone Marrow Collection General
Clippers
Surgical scrub
Lidocaine
Syringe and needle
Sterile gloves
Scalpel blade (No. 15 adequate)
Bone marrow needle
Therapeutic
13-gauge bone marrow needle
Heparin
60-mL sterile syringes
Diagnostic
Bone marrow needle: ≥16 gauge, iy2 inches
10- to 20-mL sterile syringe
Glass slides
Jar of formalin for core biopsy
Optional:
Anticoagulant
EDTA blood tubes
Petri dish or watch glass
EDTA, Ethylenediaminetetraacetic acid.
midway between the two tuberosities of the tuber coxae and somewhat toward its posterior border. With regard to angle, the needle should be pointing at the coxofemoral joint of the opposite side.
Bone marrow will be hit when the needle is inserted approximately /8 inch for foals, whereas in adult horses bone marrow may be more than 2 inches deep. The main benefit of using this method is that there is no risk of inadvertently entering the thoracic cavity.16
Preparation for Bone Marrow Aspiration or Biopsy
Bone marrow aspiration should be performed as a sterile procedure. After the animal has been restrained and the site of approach has been identified, hair should be clipped and the area surgically scrubbed (see Fig. 28.12, A). Local anesthetic is injected at the site where the needle will be inserted, from the skin to the periosteum (Figs. 28.14, B and 28.15, A). A small stab incision is typically made with a scalpel to aid the needle's approach to the bone. If the rib is to be sampled, the scalpel blade can be held in place to act as a guide for the needle. It is important to be organized and have all supplies ready so that the procedure will flow smoothly and the sample will not clot before it can be processed (Box 28.2; Fig. 28.16).
How the sample ultimately will be handled will dictate some of the available supplies needed: syringes, glass slides, Petri dish, EDTA blood tubes, and/or anticoagulant. One option is to prime the syringe that will be used for aspirating the sample with anticoagulant. Syringes are primed with heparin for therapeutic bone marrow harvesting. To prevent clotting in diagnostic samples, 1 to 2 mg of EDTA is recommended per milliliter of blood. One to two drops of a 3% to 15% EDTA solution should be adequate. The EDTA solution can be aspirated from a purple-topped blood tube. Priming the syringe with anticoagulant, although it adds a preparatory step, decreases the worry that the sample will coagulate and allows more time for processing the sample. If the syringe is not primed, as soon as the sample is seen in the syringe hub, the syringe needs to immediately be disconnected from the needle and the sample quickly processed before it has a chance to clot. If a reticulocyte count is to be performed to assess erythroid regeneration, supravital stains, such as new methylene blue and brilliant cresyl blue, require mixing with a portion of anticoagulated, liquid sample before slides are made; therefore placing at least some of the bone marrow sample in an EDTA tube is recommended.
The diagnostic sample in the syringe may be processed by expressing it directly onto several clean glass slides, into an EDTA blood tube, or into a Petri dish or watch glass. The Petri dish or watch glass must contain anticoagulant if no anticoagulant was used in the syringe. The anticoagulant commonly used is EDTA, which can be used in solution or as a salt, but other anticoagulants such as sodium citrate are also effective. Samples placed in an anticoagulant should be gently mixed immediately.
Collecting the Sample
The goal of bone marrow aspiration is to obtain a good sample of hematopoietic cells with minimal blood contamination. Anatomically, within the bone marrow, hematopoietic cells are extravascular and found in spaces dissected by venous sinuses and a central vein.30 To collect the sample, a bone marrow or spinal needle with stylet should be used. Commonly used needles include Rosenthal, Illinois sternal-iliac, and Jamshidi bone marrow needles (Fig. 28.17). Some needles come with a guard that can be adjusted to prevent deeper penetration than desired. The needle used should be 16 gauge or larger and at least 1J2 inches long. Larger needles may be needed, depending on the site of aspiration and the age and size of the animal. For therapeutic collection, a 13-gauge bone marrow aspiration needle is recommended.
After an animal has been properly prepared, the bone marrow needle is inserted through the skin, perpendicular to the bone. Once the needle contacts bone, it can be advanced using manual pressure and a clockwise-counterclockwise twisting motion (see Fig. 28.14, C). One hand can be used to stabilize the needle angle and placement while the other hand is on the needle hub pushing and turning the needle.24 If the needle is
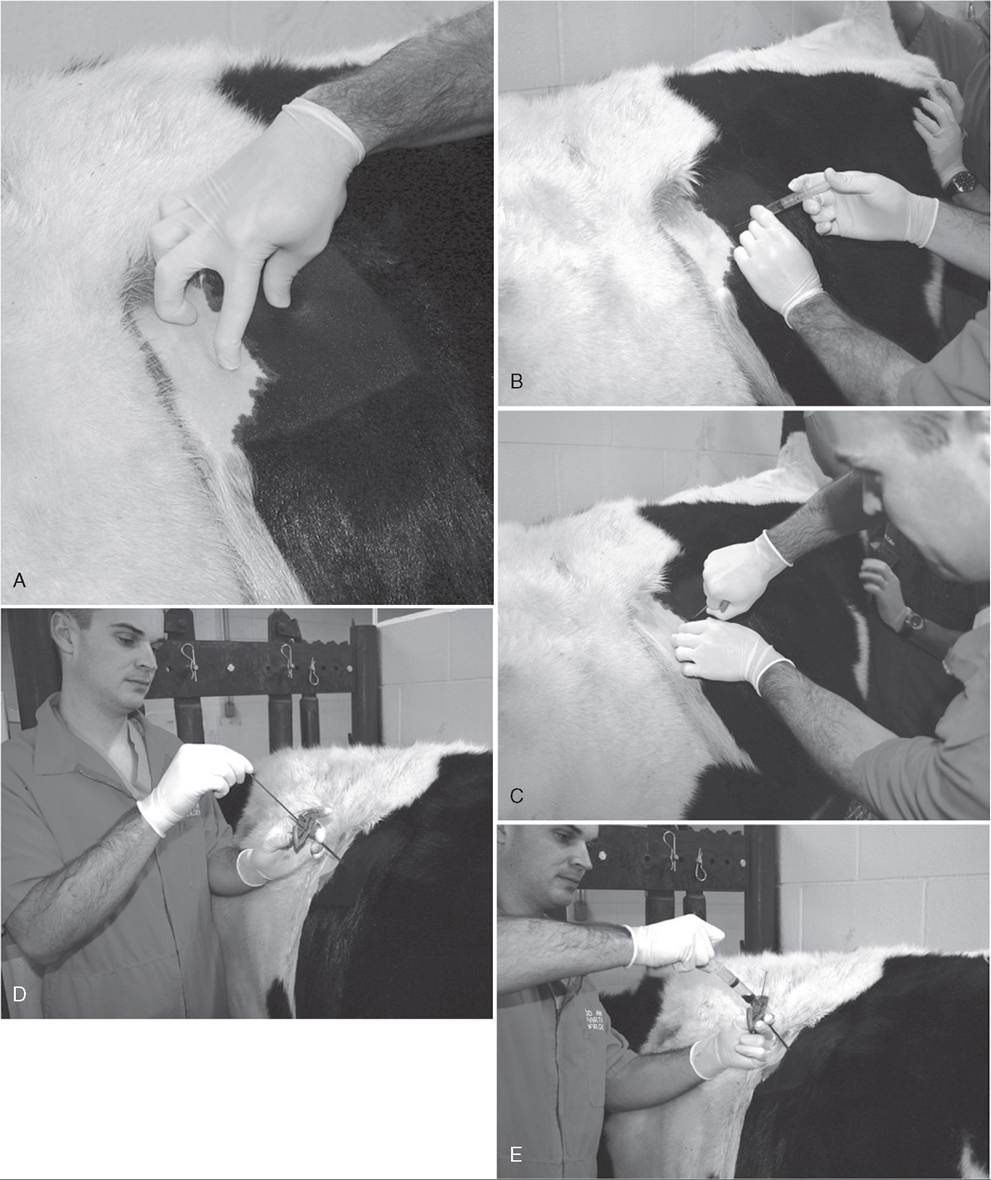
FIG. 28.14 Bone marrow aspirate of a cow. The animal was placed in a head gate and sedated, and a tail jack was applied. A, The area over the vertebral end of rib 11 has been clipped and surgically scrubbed. The cranial and caudal edges of the rib are palpated approximately 3 inches down from the costovertebral junction, and the midpoint of the rib is identified for aspiration location. B, At the chosen aspiration site, lidocaine is injected from skin to periosteum. C, After a stab incision has been made and the Jamshidi-type bone marrow needle has been inserted through the skin, the needle is forcibly pushed forward through cortical bone as it is rotated in a clockwise-counterclockwise motion. D, After a decrease in resistance is felt, the stylet is removed. E, A syringe is attached to the needle, and a few sharp pulls on the plunger are needed before sample is noted in the hub of the syringe.
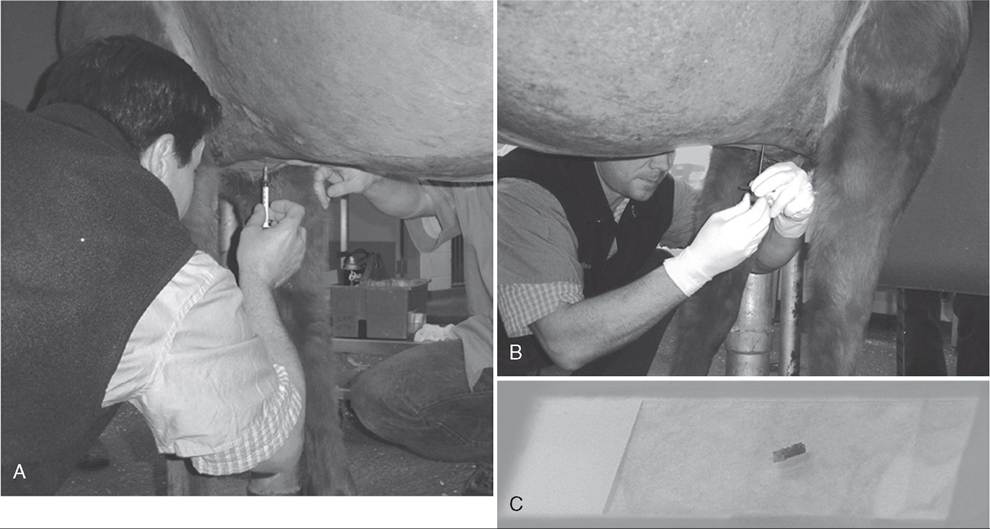
FIG. 28.15 Core bone marrow biopsy of a horse. The animal was placed in a stock and sedated; the ventral sternum between the elbows was clipped and surgically scrubbed. A, Lidocaine is injected from the skin to the periosteum. B, After a stab incision, the Jamshidi bone marrow biopsy needle is advanced into cortical bone. Here, the stylet is about to be removed before the needle is advanced further. C, Core biopsy sample.
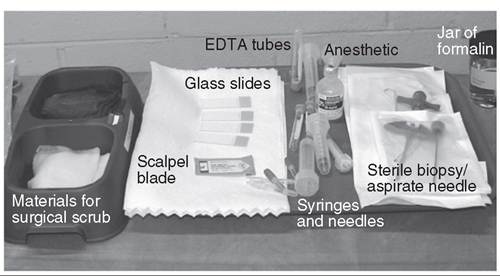
FIG. 28.16 Supply table is set up and ready for bone marrow aspiration. Sterile gloves were opened on an adjacent table. EDTA, Ethylenediaminetetraacetic acid
going through dense bone, a wood mallet can also be used to advance it.
For a diagnostic sample, once it is suspected that the needle has entered the marrow cavity, either because of detection of a sudden reduction in resistance or because of needle depth, the stylet should be removed and an aspiration attempted (see Fig. 28.14, D). In dense bone, pliers may be helpful in removing the stylet.12 After the stylet is removed, a 10- to 20-mL sterile syringe is securely attached to the needle, and the plunger of the syringe is pulled back quickly and sharply, creating negative pressure in order to dislodge bone marrow particles (see Fig. 28.14, E). Suction can be repeated two or three times. As soon as blood is seen in the hub of the syringe, suction should be discontinued, the needle and syringe removed from the animal, and the sample processed promptly. Additional suction will likely result in only dilution of the sample with peripheral blood. The first drop of blood is the most cellular, and further aspiration results in lower cellularity of the sample.31

FIG. 28.17 Bone marrow needles with stylets separated. On the left is a 14-gauge, 234 -inch Rosenthal needle. On the right is an 11-gauge, 4-inch Jamshidi needle.
For collection of equine therapeutic bone marrow, the needle is seated firmly into the center of the medullary cavity of the fifth sternebra (see Fig. 28.4). Once the needle is inserted approximately 3 to 5 mm into the bone, the stylet is removed and aspiration can begin (see Fig. 28.12, B). One or two 60-mL syringes with 10 mL each of heparin (1000 IU∕mL) are used for aspiration. The syringe is then capped, and the sample is mixed thoroughly by rocking the syringe gently back and forth. Studies have shown that the first 5 mL of an aspirate contain the highest proportion of BMSCs.22,23 Furthermore, for sequential aspirates (two aspirates of 50 mL each), the second aspirate yields few to no BMSCs.22
If the initial aspiration does not obtain any material, remove the syringe, replace the stylet, and carefully advance the needle a little further. If still no sample is obtained after additional advancement of the needle and repeated suction, slowly withdraw the needle while applying suction to the syringe. Ultimately, repositioning the needle to a different site, such as moving a couple of centimeters cranially or caudally, may result in a successful aspiration.13 It has been reported that the use of a multidirectional bone marrow aspiration needle improves the colony-forming unit fibroblast counts in a bone marrow aspirate.32
Processing the Sample for Diagnostic Purposes Whether the bone marrow sample is directly applied to glass slides or expressed into a Petri dish or watch glass, processing needs to proceed rapidly to prevent clotting or drying out of the sample. When on the slide, if the sample contains a lot of excess blood, the slide can be briefly tilted so that the fluid portion can run off into an absorbent surface, leaving behind adherent particles for spreading (Fig. 28.18, C and Fig. 28.19, A). If the sample is placed into an EDTA tube or Petri dish with anticoagulant, spicules (small grayish particles) can be transferred out of the bloody sample using a pipette and placed on a glass slide20 (see Fig. 28.18).
To spread the sample on a slide, place a second glass slide flat on top of the sample, allowing the sample to form a thin layer between the slides (Fig. 28.19, B). Without additional pressure other than the weight of the slide, gently pull the slides apart from each other horizontally and without vertical separation, which can create suction and rupture cells (Fig. 28.19, C). This typically results in a nicely spread sample with intact particles and nice monocellular layers for evaluation. Several slides should be made. After slides are made, they should be allowed to air dry, kept away from formalin fumes, and stored at room temperature until staining.
Some bone marrow slides are stained with a Romanowsky- type stain (Wright, Giemsa, Diff-Quik) for cytologic examination, and some should be left unstained in the event that special staining procedures are wanted. It is highly recommended that at least one slide be stained right away for microscopic examination in order to determine sample quality and to ensure that bone marrow elements are present while the animal is still available and prepped, in the event that the first aspiration is nondiagnostic and additional attempts will be needed (Fig. 28.20). If a sample containing mostly peripheral blood without spicules is obtained, it may be possible to acquire diagnostic information by centrifuging the sample in Wintrobe hematocrit tubes and making smears from the buffy coat. Staining for reticulocytes requires that an anticoagulated, liquid bone marrow sample be mixed and incubated with a supravital stain before slides are made.
If a core biopsy sample is obtained, the tissue can be gently rolled on a slide to make an impression smear for cytologic evaluation. The biopsy tissue should then be placed in 10% neutral buffered formalin for preservation. A larger gauge needle (10 to 13 gauge) is generally recommended for core biopsy. The Jamshidi needle, designed so that the distal tip tapers to help retain the sample, is the most popular needle for biopsy. The needle and stylet are initially inserted as for
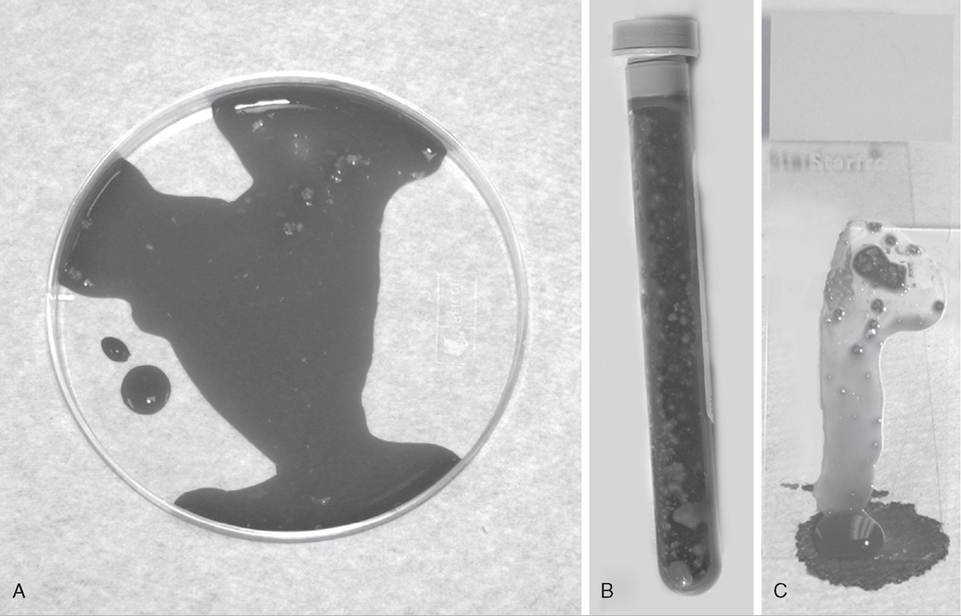
FIG. 28.18 Bone marrow spicules (small grayish particles) should be seen in the aspirated sample. A, Particles can be picked out of background blood from a Petri dish. B, Particles can be seen adhering to the sides of an ethylenediaminetetraacetic acid (EDTA) blood tube. C, Particles will adhere to a glass slide while excess blood runs off.
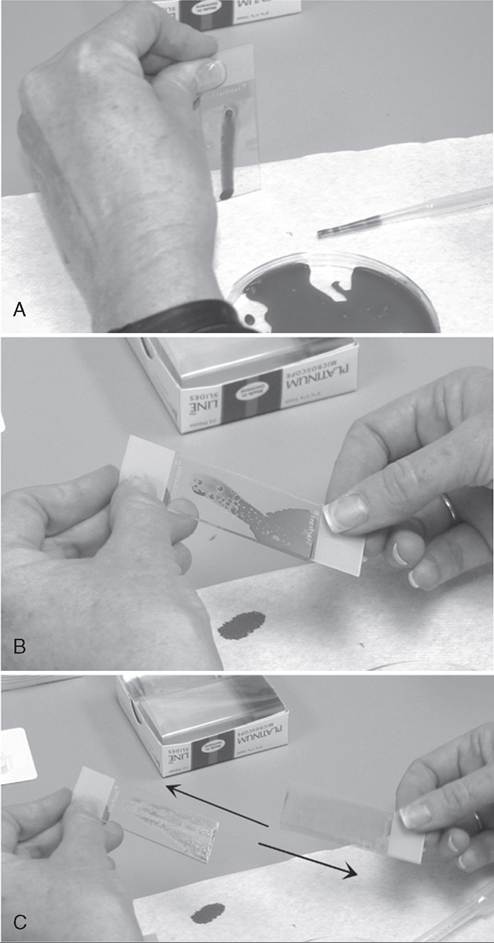
FIG. 28.19 Making slides of a bone marrow sample. A, Excess blood is allowed to run off the slide onto an absorbent surface while the spicule remains adhered to the slide. B, A second slide is laid on top of the sample, causing the sample to spread out between the slides. C, The slides are horizontally pulled apart, then allowed to air dry.
aspiration (see Fig. 28.15, B). Once the needle enters the bone marrow, the stylet is removed and the needle is advanced further with the same twisting motion. Ideally, the needle is inserted at least an additional 1 to 2 cm, but this may be limited by location. After the needle is advanced to obtain the core, it is rotated and rocked forcibly to help break the core at its base for successful removal. Once the needle is removed from the animal, a probe is inserted into its lumen at the distal tip, pushing the sample out the hub end (see Fig. 28.15, C).
Often bone marrow aspirates are placed into an EDTA blood tube for submission to an outside laboratory. In this case it is still recommended to make slides of the sample to submit along with the fluid sample. If the sample is left in the fluid phase, cells can deteriorate during transit, and it is always helpful for the cytologist to have a freshly prepared sample to
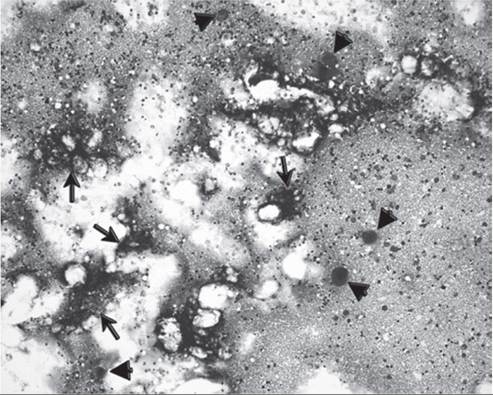
FIG. 28.20 Stained slide of adequate bone marrow aspirate sample. Megakaryocytes (arrowheads) and particles (arrows) are present. There is also increased cellularity compared with peripheral blood. (Wright-Giemsa stain, 10? objective.)
examine (of both bone marrow and peripheral blood). In addition, a slide can be stained and evaluated for diagnostic quality before the sample is shipped.
If repeated aspirates all result in samples of low cellularity, a core biopsy is typically indicated. Cytologically, it can be impossible to differentiate low cellularity caused by a pathologic process from that resulting from poor sampling; therefore a biopsy is used to evaluate cellularity.
Processing the Sample for Therapeutic Purposes
Bone marrow aspirates and concentrates have the advantage of being immediately available for injection after collection with minimal processing. However, multipotent stromal cells represent a minor fraction of the total population of nucleated cells in these samples. The other cells that comprise the aspirate include hematopoietic cells, monocytes and macrophages, and low numbers of lymphoid cells and endothelial progenitors. Studies suggest that after density centrifugation, which removes granulocytes and immature myeloid precursors, BMSCs are only 0.001% to 0.01% of the mononuclear cells remaining.33,34 Concentrated bone marrow is made by centrifuging the heparinized bone marrow aspirate sample at 1500 revolutions per minute (rpm) for 10 minutes and removing the supernatant. In concentrated bone marrow, platelet and leukocyte concentrations increase (~8 times), but erythrocyte concentration decreases.35
Because BMSCs comprise such a small proportion of bone marrow, techniques have been developed for their selection and isolation. Commercial closed systems are available to separate MSCs. These kits can optimize cell viability after collection and reduce the risk of contamination36 (PrepaCyte-CB, U.S. Patents 6,933,148 and 7,160,723). Studies in humans have shown that these closed systems provide a fast and reliable separation of human cord blood, with higher recovery rates of nucleated cells compared to other methods. Although this method removes most red blood cells, the addition of ammonium chloride solution to lyse the remaining red blood cells is recommended. The remaining nucleated cells are washed with a buffered isotonic media (Dulbecco's phosphate-buffered saline [DPBS]) and spun at 2100 rpm for 5 minutes. After the supernatant is discarded, the cells are resuspended in growth media. Another commonly performed open isolation method for enriching nucleated cells is to place the bone marrow aspirate in a density gradient solution for separation of the mononuclear fraction by centrifugation, prior to culture in growth media. Two density gradient solutions, Percoll and Ficoll, are commonly used for this method. A study performed with equine bone marrow showed that Percoll solution may have a higher yield of BMSCs and earlier self-renewal (14 days) than Ficoll solution.37 This same study also compared both density gradient solutions to a classic isolation method based on MSCs from bone marrow concentrates adhering to plastic culture dishes, and no significant difference in cell viability or in osteogenic or chondrogenic differentiation was identified between the protocols.37
More on the topic Bone Marrow Collection:
- Bone Marrow Collection
- Bone Marrow Evaluation
- Basic Caprine Hematology
- Myeloid and Megakaryocytic Bone Marrow Hypoplasia
- Lymphoma in Horses
- REFERENCES
- Bone marrow is composed of hematopoietic cells as well as structural components, including trabecular bone, adipose tissue, a sinusoidal system, supporting reticular cells, and an extracellular matrix.
- Immunosuppression Associated With Leukoproliferative Disorders*
- Evaluation of the Anemic Patient
- Interpretation of the Ieukogram in the context of the clinical history, the physical examination, and the rest of the minimum laboratory database (complete blood cell count, serum biochemical data, and urinalysis) can provide valuable insights into the diagnostic process in large animal species.