Clinical Examination ofthe
Respiratory Tract
Either a well-taken case history or a basic physical exam may suggest the presence of respiratory disease. Signs noted might include increased respiratory rate, labored breathing, rapid tiring (especially with exercise), cyanosis, abnormal sounds associated with breathing, nasal discharge, coughing, or fever.
Table 9.1 lists some of these signs and possible etiologies.If a respiratory disease is suspected, additional herd history is helpful in directing the diagnostic efforts. The owner should always be questioned concerning recent purchase or boarding of animals or attendance at shows, relative to possible introduction of infectious diseases. Do the goats get out of the barn, at least during part of the year? If not, lungworms and nasal bots are less probable. Is the herd
Table 9.1 Some signs suggestive of respiratory disease and possible causes.
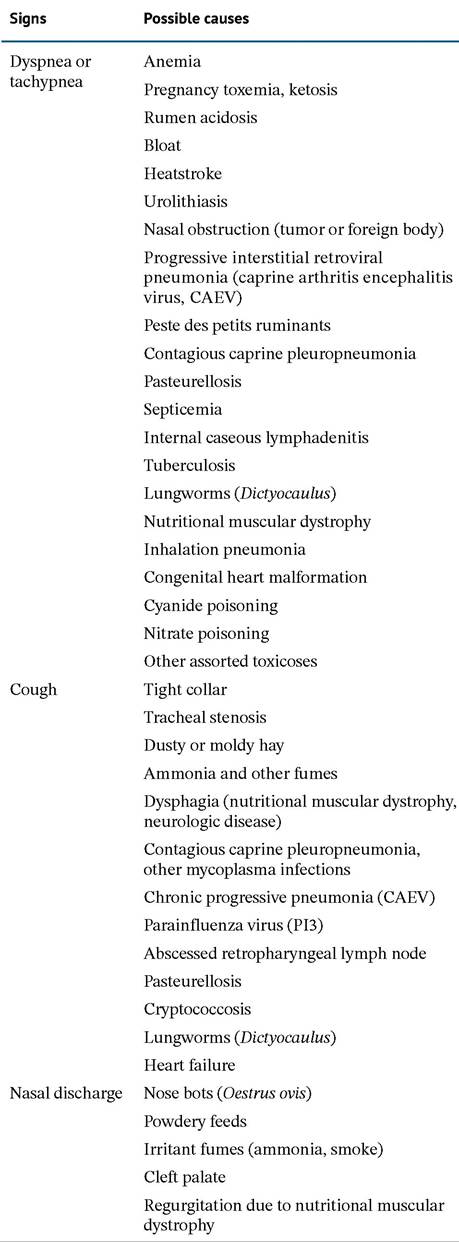

Figure 9.1 Normal goat lung with trachea opened to demonstrate the tracheal bronchus supplying the right cranial lobe. Source: Courtesy of Dr. M.C. Smith.
Table 9.1 (Continued)
Signs Possible causes
Atrophic rhinitis (toxigenic stains of Pasteurella multocida)
Nasal adenocarcinoma
Paste des petits ruminants Parainfluenza virus (PI3) Respiratory syncytial virus Caprine herpesvirus Pulmonary adenomatosis (jaagsiekte) Mycoplasma infections Pasteurellosis
Melioidosis
Cryptococcosis
Note: The list is incomplete.
known to be infected with or believed to be free of caprine arthritis encephalitis (CAE) virus, caseous lymphadenitis, and mycoplasma mastitis? Are housing and ventilation acceptable? The veterinarian should not accept the owner's answer to this last question without personally inspecting the premises.
Is the region selenium deficient, and is the ration supplemented with vitamin E and selenium? Has the animal been overdosed with injectable selenium, so that it is dyspneic because of heart failure?It is often impossible to obtain an exact and unquestionable etiologic diagnosis, at least in the living goat. This frustrates recent graduates, whose education has suggested that the clever clinician always gets the right answer. On the other hand, more “experienced” practitioners may prescribe an antibiotic that has worked well for pneumonia cases seen previously, rather than try to determine the cause of the clinical signs observed in every animal. Veterinarians often supply larger farms under their care with treatment protocols that specify the first-choice antibiotic and additional drugs to use in the event of treatment failure. Goats that fail to respond should receive a careful physical examination and/or a necropsy to allow refinement of the protocols.
Not every goat that breathes rapidly or “harshly” has respiratory disease. A complete physical examination always helps avoid embarrassing misdiagnoses. If the mucous membranes are white, think first of anemia, not pneumonia. Do not waste the owner's money on tracheal washes and expensive antibiotics if the kid has an obvious heart murmur, at least not without explaining the seriousness of the underlying heart disease.
Common pulmonary function tests have been adapted to the goat and normal values published (Bakima et al. 1988, 1990). This information should be useful to researchers evaluating respiratory disorders in goats or using goats as models in the study of respiratory physiology.
Respiratory Rate
The normal respiratory rate at rest is approximately 10-30 breaths per minute (kids 20-40 per minute). Few goats are “at rest” in the presence of an odoriferous stranger or after a long ride to the clinic in the back of a compact car. In addition, many normal goats pant; a respiratory rate of 270 per minute has been reported for goats held at 40 °C (104 °F).
A goat with a long winter coat will certainly breathe rapidly if brought into a warm and humid room. A curious goat, continually sniffing the examiner, makes just the counting of the respiratory rate frustrating or even meaningless. The movements of the chest and abdominal wall should be observed from a distance, before the patient is disturbed. This is also the best time to note normal costo- abdominal respiration, abdominal pumping, or very shallow and painful chest movements (as with pleuritis).Many seriously ill goats have an increased respiratory rate because of fever, metabolic disturbances, or pain. Pregnancy toxemia, lactational ketosis, rumen acidosis, or diarrhea can all lead to metabolic acidosis. As part of the respiratory compensation mechanism, goats breathe faster to release carbon dioxide and thereby remove H+ (along with HCO3-) ions from the blood. Goats with listeriosis or other brain stem disease, on the other hand, may have an altered respiratory rate because of acidosis from loss of saliva or lesions in the respiratory centers of the brain. Metabolic alkalosis, which may be accompanied by very slow respiration, is less common in goats than in cattle, because most conditions associated with abomasal stasis (e.g., impaction, displacement, torsion, ulceration) are relatively rare.
Dyspnea
It is helpful to differentiate difficulty in breathing into inspiratory, expiratory, or mixed dyspnea. Strong outward movements of the thorax and longer inspiration are associated with inspiratory dyspnea. Narrowed upper airway passages or bronchopneumonia with reduced respiratory surface in the lungs causes such a pattern. A distended head and neck and dilated nostrils accompany severe inspiratory dyspnea, and audible stenotic sounds may make location of an obstruction possible. With expiratory dyspnea, breathing out is impeded and is accentuated by strong and prolonged expiratory movements of the abdomen. This is less common in goats than in cattle, because the caprine lung is not predisposed to interstitial emphysema.
Cheek blowing or open-mouth breathing with an extended tongue might accompany expiratory dyspnea. Logically, a mixed dyspnea occurs when there is difficulty in both inhaling and exhaling.Whenever the dyspnea is accompanied by cyanosis, the examiner should proceed cautiously to limit additional stress to the goat. If an upper airway obstruction is suspected, an emergency tracheostomy may become necessary; this can be performed by cutting between two rings in the midcervical region, but a small-diameter tube will be needed. The heart must also be examined closely, because the cause of dyspnea may reside in the circulatory rather than respiratory system.
Externally Audible Sounds
Sneezing, a brief and powerful expulsion of air through the nose, occurs when the nasal mucosa is irritated by accumulations of secretions, exudates, or foreign matter. Stenotic sounds are caused by constriction in the upper respiratory tract. Snuffling sounds of nasal origin are usually loudest on inspiration. Alternate occlusion of one nostril and then the other helps to determine if the stenosis is unilateral or bilateral. That is, with a unilateral lesion, blocking the nostril on the affected side should decrease the sound, while blocking the other nostril should increase the sound by forcing more air through the stenotic nasal passage. Sounds of pharyngeal origin are loudest on expiration, whereas laryngeal stenosis sounds are usually more pronounced on inspiration. Manual compression of the pharynx increases the loudness of low-pitched stertorous pharyngeal sounds while decreasing high-pitched laryngeal stridor. Sounds originating from a stenotic larynx are accentuated by additional compression of the larynx. If the stenosis is in the trachea, occlusion of one nostril or compression of the pharynx or larynx decreases the air flow and the loudness of the stridor. Auscultation along the accessible portion of the trachea may permit localization of the lesion. The character of any stenotic sound (i.e., whistling, hissing, sawing) may be affected by the presence or absence of exudate in the airways.
Coughing
A cough may simply indicate irritation from fumes or dusty feed or compression of the trachea during attempts to reach something theoretically out of reach, such as the neighbor’s feed. If irritation lies in the upper respiratory tract, the cough is typically dry and powerful. If the goat has a deep-seated bronchopneumonia, the cough may be moist and feeble. Coughing can be elicited by first briefly preventing respiration. This is done by holding a gloved hand or moist towel or similar object over the nostrils until the goat becomes distressed. When the nose is released, the number and nature of coughs are noted and the lungs are auscultated for abnormal respiratory sounds, often accentuated by this procedure.
Nasal Discharge
Possible causes of a nasal discharge are listed in Table 9.1 or discussed under the topic of rhinitis below. Figure 9.2 shows a goat with a mucopurulent nasal discharge during a herd outbreak of infectious keratoconjunctivitis, possibly due to Mycoplasma conjunctivae (see Chapter 6). A purulent secretion is more significant than a serous discharge. A clear scanty bilateral nasal discharge is not unusual in adult goats in apparent good health. Clinically normal goats also harbor a wide variety of aerobic bacteria in their nasal passages, including Pasteurella multocida, Mannheimia haemolytica, and Streptococcus spp. (Ngatia et al. 1985).
Closer Examination ofthe Upper
Respiratory Tract
It is useful to smell the breath; rotten odors may suggest the presence of infection or tumor in a sinus or along the airways. Compare with the smell of the open mouth. Some clinicians have the ability to detect ketone bodies on the breath, as in an animal with pregnancy toxemia; those who do not should keep a container handy to catch urine, because the goat typically urinates on arising or after the stress or insult of close physical examination. If asymmetry

Figure 9.2 Feed particles adhering to a mucopurulent nasal discharge.
Source: Courtesy of Dr. M.C. Smith.in airflow from the two nostrils is detected while smelling the breath or by holding the palm of the hand before each nostril, a tumor or foreign body may be present.
The frontal and paranasal sinuses may be the source of foul odors and should be externally palpated and percussed. If the goat is hornless, the time and method of dehorning should be ascertained. If the goat does not eat hay and chew its cud freely, a tooth root abscess rather than a problem in the respiratory tract may be the source of a bad odor. Radiography may be helpful for diagnosing infections or tumors of the sinuses.
When lesions in the pharynx or larynx are suspected, direct visualization is desirable. Light sedation with xyla- zine permits a good view of the back of the throat and the teeth. Manual exploration without sedation is hazardous at best. Naturally, in regions where rabies occurs, great care should be taken in all aspects of the physical examination.
Do not neglect to palpate very carefully for the retropharyngeal lymph nodes. Their enlargement may occur with non-specific local infections, but is more common with caseous lymphadenitis. A progressive dyspnea occurs because of external compression of the airway (Jones and Schumacher 1990). Capripox infection can cause a similar obstructive lymph node enlargement in countries where this disease exists (Kitching 2004). When the nodes are enlarged, great care should be taken to avoid extending or flexing the neck during restraint for physical examination or diagnostic procedures; the increased compromise of the airway may be rapidly fatal.
Endoscopic examination of the nasal passages, pharynx, larynx, and trachea has been performed in awake, untran- quilized adult goats using a 4 mm flexible endoscope and illustrations of findings in normal animals published (Stierschneider et al. 2007). These authors report that the normal goat's trachea may be drop shaped, round, or U-shaped in cross-section. This suggests that one case report of tracheal collapse in a goat (Belli et al. 2003) might have been a misdiagnosis at necropsy.
The trachea of a goat may be partially obstructed by a mass protruding into the lumen or by tracheal collapse. Coughing, stridor, and exercise intolerance are to be expected. Refrain from diagnosing a hypoplastic trachea without close comparison with healthy goats of the same age and size. That the caprine trachea is relatively small in diameter is well substantiated by the size of endotracheal tube typically required (see Chapter 17). Radiographic evaluation should be helpful in confirming stenotic tracheal lesions or compression from enlarged lymph nodes (Jones and Schumacher 1990). If localization of the problem is possible, excision of a mass or even placement of prosthetic tracheal rings may be attempted (Jackson et al. 1986). In one young kid, tracheal collapse resolved after the inciting bronchopneumonia was successfully treated (Corbera et al. 2009).
In confined groups of animals, a head tilt, sometimes accompanied by facial nerve paralysis, suggests the possibility of bacterial pneumonia. This is because organisms responsible for pneumonia can also ascend the eustachian tube and cause an otitis media/interna.
Auscultation ofthe Lungs
Much disagreement exists in the literature regarding terminology for normal and abnormal lung sounds. In addition, harsh inspiratory sounds may be heard over the entire lung field of a goat, especially a thin one, whether the lungs are normal or extensively altered by disease processes. The duration of expiration is also audible in goats, as in sheep. Special efforts should be made to auscultate well forward under the shoulder and elbow, where cranioventral pneumonias are localized.
Normal breath sounds are loudest on inspiration and over the trachea and base of the lungs. They are bronchial sounds; the velocity of airflow in alveoli is too low to generate audible sounds, and thus the terms “bronchovesicular” and “alveolar sounds” are inappropriate (Curtis et al. 1986). Increased breath sounds are heard in normal animals with increased rate and depth of respiration (i.e., excitement, exercise, high environmental temperature) or in goats with fever, acidosis, or pulmonary congestion.
“Increased bronchial sounds” are heard on both inspiration and expiration. They occur in disease processes when the bronchial lumen remains open, but the surrounding lung tissue transmits sound better because of being consolidated. This is true of most pneumonias of goats. There is no sharp line of demarcation between increased breath sounds and increased bronchial sounds. Crackles are clicking, popping, or bubbling sounds produced by fluid in the airways or by dry airways suddenly popping open. The term “crackles” can be used in preference to “moist rales” because it does not erroneously imply anything about the amount of fluid in the airways. Wheezes (also called rhon- chi or dry rales) are whistling or squeaking sounds typically caused by the passage of air through a narrowed airway. Bronchospasm, abscesses, and tenacious exudate are possible causes of wheezes. Both crackles and wheezes may stop or move to another location, as when coughing dislodges fluid or exudate. Stridors (loud, wheezing-type sounds loudest over the trachea or larynx) may be referred to the lung fields, but they result from stenosis in the upper respiratory tract and are commonly audible without a stethoscope.
Pleuritic friction rubs, described as “sandpaper-like sounds,” occur with severe inflammation of the pleura, assuming that adhesion or effusion does not prevent the rubbing.
The absence of breath sounds may be simply because of obesity, as in some Nubians. Pleural effusion, pneumothorax, diaphragmatic hernia, and space-occupying thoracic lesions (thymoma) are other possibilities. Breath sounds may be decreased with shallow breathing from pain, weakness, or central nervous disorders (Curtis et al. 1986).
Lung auscultation findings in normal sheep and sheep with specific respiratory tract diseases have been reviewed, with supplemental recordings available online (Scott 2010); these recordings should also be relevant to auscultation of goat lungs.
Percussion of the Lung Fields
In the past, the technique of finger-finger percussion or the use of a pleximeter has been more popular in Europe than in America. Thoracic percussion has been reviewed (Roudebush and Sweeney 1990). Veterinarians who expect to obtain useful diagnostic information from the procedure should routinely percuss many goats to become familiar with the normal sounds and lung boundaries. Percussion is usually done on the right side, although the presence of the spleen on the left makes it possible to identify the upper border between lung and rumen. The caudal lung border normally extends in an arc from the dorsal aspect of the eleventh intercostal space to the point of the elbow. A prescapular percussion field is present, and in thin animals the lungs can be percussed through the ventral portions of the scapula. Lifting a flexed forelimb to the side permits clearer percussion of axillary areas (Marek and Mocsy 1960). The full resonance of normal lung is to be contrasted with the more tympanic sound of gas-filled rumen or intestine, the relatively damped or dull sound of ventral abdominal organs, and the absolute dullness of the liver (on the right). A duller than normal sound over the lung fields can occur when large areas of the lung are consolidated by abscess, tumor, or interstitial pneumonia. The dull area is ventrally located and has a horizontal dorsal border if accumulation of fluid in the thorax is responsible. Processes causing increased intra-abdominal pressure (including late pregnancy) can displace the lung borders in a cranial direction.
Blood Gas Measurement
When laboratory testing is accessible, standard blood gas measurements give an indication of pulmonary function, as well as the acid-base status of the animal. Venous blood is routinely collected in heparin, avoiding contamination of the sample with room air. Few studies specific to the goat have been published, and ideally each testing laboratory should determine the reference ranges for the apparatus being used, because some variability is to be expected (Kahrer et al. 2006). Time and temperature of blood storage before testing also influence test results. For instance, there is a slight decrease in concentration of HCO3- and a marked increase in pO2 with storage for 24 hours at 4 °C (39 °F), while pH is stable (Piccione et al. 2007). Blood gases determined by Blood Gas Analyzer on 29 adult goats, one each from 29 farms, are presented in Table 9.2 (Stevens et al. 1994). Respiratory acidosis, with increased pCO2 and HCO3-, is expected with impaired pulmonary function.
Transtracheal Aspiration
The small diameter of the trachea makes this a more difficult procedure in goats than in cattle.
Indications
Transtracheal aspiration is useful for obtaining samples for cytology and bacteriologic culture in the diagnosis of an etiologic agent. Microbial sensitivity testing aids the choice of antibiotics to be used in treating a particularly valuable goat or one that has failed to respond to previous rational therapy. The use of sensitivity testing also may help to lessen the development of antimicrobial resistance. The frequency of recovery of pathogens from the trachea of goats when pulmonary disease is absent is unknown. Cultures from nasal swabs are of no diagnostic value relative to bacterial pneumonia.
Technique
The hair is clipped midway over the cervical trachea and a small bleb of local anesthetic is injected beneath the disinfected skin. Sterile gloves should be worn. A 14-gauge needle is used to penetrate the trachea and a 3 French polypropylene catheter or a 3.5 French tomcat catheter is passed into the trachea. A 16- or 18-gauge intravenous (IV) catheter device may be used instead. The needle portion
Table 9.2 Blood gases of adult goats determined on venous blood.
| Parameter | Mean | 2.5 percentile | 97.5 percentile |
| pH | 7.38 | 7.30 | 7.50 |
| pCO2 (mmHg) | 40.6 | 34.6 | 48.8 |
| HCO- (mmol/L) | 25.0 | 19.6 | 29.4 |
| TCO2 (mmol/L) calculated | 26.2 | 20.7 | 30.7 |
| pO2 (mmHg) | 48.8 |
Source: Modified from Stevens et al. 1994.
should be withdrawn after placement of the catheter into the trachea to avoid cutting off part of the catheter. Sterile, buffered saline (15-20 mL) is injected into the trachea. At once, as much as possible (often only a few milliliters) is aspirated into the syringe and submitted for microscopic examination and culture. The catheter is then removed. No special aftercare is needed.
A different technique has been described in standing adult sheep with the head restrained in a slightly elevated position (Sheehan et al. 2005). The site for catheter placement is approximately 5 cm distal to the larynx. A 12-gauge 52 mm IV catheter is inserted between two tracheal rings and directed toward the lungs after the needle is retracted. A 1.7 mm (5 French) polyethylene male-to-female luer lock suction catheter cut to a length estimated to enter the lungs (measured to a point behind the shoulder) is then introduced into the trachea through the first catheter. Infusing 30 mL of sterile saline allows recovery of approximately 10 mL of fluid five seconds later.
Bronchoalveolar Lavage
In a hospital or research setting, better samples for cytology are obtained with the goat sedated (acepromazine at 0.3 mg/kg IV) or under general anesthesia and intubated. A tracheal wash catheter is passed through the endotracheal tube to the bronchial bifurcation. In an adult goat, approximately 50 mL of warm sterile saline is flushed into the lungs and then aspirated at once through the same catheter (Berrag et al. 1997). Recovery of fluid would probably be improved by use of a pediatric bronchoscope, if available. The authors report that in normal goats the predominant cell type recovered is alveolar macrophage (80-95%), with fewer lymphocytes, eosinophils, neutrophils, and epithelial cells. The lavage findings for goats with various forms of pneumonia have been reported by Jarikre et al. (2016). Numerous eosinophils would raise the suspicion of parasitic disease.
Radiographyofthe Lungs
Radiography can document the presence of cranioventral bronchopneumonia, interstitial pneumonia, pleural effusion (often marked in contagious caprine pleuropneumonia, CCPP), a penetrating metallic foreign body, thymoma, tracheal compression by enlarged mediastinal lymph nodes, or underlying cardiac disease leading to respiratory signs (Ahuja et al. 1985). The value of pulmonary radiographs often comes from confirmation of advanced and extensive changes in the lung fields. Multiple abscesses or massive areas of interstitial pneumonia suggest a very grave prognosis. Sternal and mediastinal lymph nodes should be examined for evidence of enlargement. Sternal abscesses with penetration into the thorax are accompanied by visibly enlarged sternal nodes and often by osteomyelitis of the sternebrae. Both viral and bacterial pneumonias, if chronic, can result in enlargement of mediastinal nodes.
A large thymoma may displace the lungs caudally. Because many thymomas in goats are incidental findings at necropsy (Hadlow 1978), it is conceivable that an asymptomatic tumor might be identified during radiography of a goat with some other thoracic disease. If the lungs are displaced cranially, consideration should be given to a (very rare) diaphragmatic hernia (Tafti 1998).
The radiographic equipment and techniques used for dogs are also appropriate for goats. The forelimbs need to be pulled well forward to expose the cranioventral lung lobes. Light tranquilization (see Chapter 17), combined with clever use of tape and sandbags, provides safe restraint. Avoid xylazine (normally effective at 0.05 mg/kg IV) if the animal is already dyspneic or cyanotic.
Ultrasonography of the Thorax
The physical or chemical restraint needed to obtain diagnostic radiographs of the chest may be dangerous to a severely dyspneic animal. Ultrasound examination can be done in a standing animal, usually at less expense than radiography. Scott and Gessert (1998) have described the procedure for sheep, and their findings should be applicable to goats. A sector scanner transducer rather than a linear array transducer is preferred because of the narrow intercostal space, and examination may not be possible in small goats. Hair is clipped from a 7 cm wide strip of skin caudal to the scapula and elbow bilaterally. Starting in the sixth or seventh intercostal space, the thorax is examined in longitudinal and transverse planes. The front limb is adducted and the clipped skin slid forward several spaces to allow access to the ventral aspect of the chest. Examination beginning from the ninth or tenth intercostal space assesses the dorsal lung field. Liberal wetting of the hair with alcohol can be substituted for clipping and application of an ultrasound gel.
Normally aerated lung does not permit penetration of the ultrasound beam, so a bright linear echo and reverberation artifacts are all that are seen during examination of a normal animal. Ultrasound is useful for demonstrating fluid accumulation in the pleural space, abscesses that reach the pleura, tumors, and consolidation by bacterial or interstitial viral pneumonia (Scott and Gessert 1998).
Computed Tomography of the Thorax
Computed tomography measurements of the thorax of healthy goats have been reported by several authors (Alsafy 2008; Ohlerth et al. 2012). The modality is occasionally used with pet goats or in research settings.
Lung Biopsy and Aspiration of Fluid from the Thorax
If a fluid line is percussed in the thorax or detected by radiography or ultrasonography, thoracocentesis may be indicated. Clipping of hair and thorough disinfection of the skin are mandatory. A site beneath the fluid level but not directly over the heart should be chosen, and the needle should be kept close to the anterior edge of a rib to avoid nerves and blood vessels.
Percutaneous lung biopsy (fine needle aspiration) is rarely performed, but can be used to confirm the presence of an extensive interstitial pneumonia or tumor, as is associated with retroviral infections. The technique has been described in small animal medicine textbooks (Johnson 2005) and in sheep (Braun et al. 2000a).
Advanced Laboratory DiagnosticTechniques
It is often critical to obtain a rapid and accurate diagnosis of the etiologic agent that is causing respiratory disease in one or more goats. Classical bacterial and viral isolation techniques as well as histology may take too long (Chakraborty et al. 2014). Although availability will vary with the region and the laboratory, polymerase chain reaction (PCR) tests and other molecular biology techniques will speed the confirmation of the etiologic agent(s). This is especially important in a herd outbreak or when there is potential for the introduction of a transboundary disease. The laboratory should be consulted for the best tests to request, and fresh necropsies may yield the best samples.
More on the topic Clinical Examination ofthe:
- Physical Examination
- Smith Mary C., Sherman David M.. Goat Medicine. 3rd edition. — Wiley-Blackwell,2023. — 976 p., 2023
- Stomach
- Medical Record
- THE PAEDIATRIC CONSULTATION AND CLINICAL CONSIDERATIONS
- PHYSICAL EXAMINATION AND DIAGNOSTICS
- Clinical features of Lyme borreliosis in humans in Bulgaria
- Diagnosis
- Submission of Laboratory Samples
- Oropharynx