ClinicalSigns
Classically, human and animal sporotrichosis is acquired by traumatic inoculation of the fungus in the subcutaneous tissue (Barros et al. 2011; Orofino-Costa et al. 2017) and is usually associated with lymphangitis.
The inoculum load, the immune status of the host, the virulence of the inoculated strain, the depth of traumatic inoculation, and the fungus species influence the development of sporotrichosis (Rodrigues et al. 2016b; Della Terra et al. 2017).After traumatic inoculation in cats, the incubation period ranges from days to months. The domestic cat is highly susceptible to infection by S. brasiliensis. Several clinical manifestations have been reported, characterizing sporotrichosis as a polymorphic disease, which can be mistaken for a number of other dermatologic manifestations such as atypical mycobacteriosis, cryptococcosis, histoplasmosis, neoplasias, and cutaneous leishmaniasis. Feline sporotrichosis ranges from an infection with no apparent cutaneous manifestations to dissemination with or without extracutaneous signs. The lesions are ulcerative and crusty, with alopecia, and generally exhibit central ulceration (Fig. 10.8).
In cats, the disease occurs more often among males during reproductive age. This finding suggests an important relation with forays and animal fights (Schubach et al. 2001, 2002). Most skin lesions are observed in the head, the most affected area during fights. However, mucosal involvement may also occur due to cat habits such as licking, which can transfer a considerable amount of yeast cells from the skin lesions to the oral cavity, as well as to other distant body parts.
A considerable amount of yeast is present in skin lesions and exudates of cats, boosting horizontal animal transmission or zoonotic transmission. Owners of a sick animal commonly acquire sporotrichosis during oral administration of antifungals because the animal may bite or scratch, consequently, inoculating the yeast.
Therefore, care must be taken, such as using gloves and safety equipment during animal handling, to prevent the progression of the sporotrichosis transmission chain.Clinical manifestations in humans range from localized nodules and ulcers to ulcers along the lymphatic pathway, dissemination through the skin with mucosal
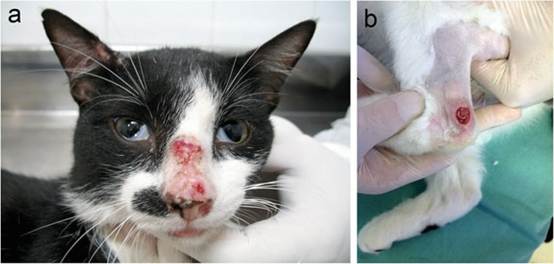
Fig. 10.8 Clinical aspects of feline sporotrichosis caused by Sporothrix brasiliensis in South and Southeast Brazil. Images of feline sporotrichosis courtesy of Dr. Sandro Antonio Pereira (INI/Fiocruz, Brazil) (right) and Dr. Flavio de Queiroz Telles Filho (Federal University of Parana, Brazil) (left)
tissue involvement, and even lung involvement. When acquired via the classical transmission route, the mycosis is more common in workers such as gardeners, vegetable growers, and farmers (Powell et al. 1978). Conidial inhalation is uncommon in sporotrichosis, but it may result in pulmonary and systemic forms of the disease, with spread to the bones, eyes, central nervous system, and internal organs; these forms mainly occur in immunocompromised patients (Kauffman 1999; Kauffman et al. 2007; Aung et al. 2013). When acquired through the alternative transmission route, the mycosis is more frequent in cat owners and veterinarians, ceasing to be an occupational hazard and exposing more individuals to the disease due to intimate contact between domestic cats and humans.
Human sporotrichosis is mostly a benign infection limited to the skin and the subcutaneous tissue, with spread to the bones and internal organs possible. The initial lesion that develops as granulomatous nodules may progress to a necrotic or ulcerative lesion. During this period, the adjacent lymphatic vessels become thick and similar to a rope. Along the lymphatic vessels, multiple subcutaneous nodules and abscesses are observed. The disease has subacute to chronic evolution in immunocompetent patients and may spread in immunocompromised patients (Silva-Vergara et al.
2012). Cases in which the fungus has reached the joints causing osteoarthritis have frequently been reported (Al-Tawfiq and Wools 1998; Koeter and Jackson 2006; Orofino-Costa et al. 2010). The mechanism and tropism of the fungus to the synovial fluid, bones, and cartilage are still unknown. Sporotrichosis lesions are often misdiagnosed as other diseases such as cutaneous leishmaniasis (Castrejon et al. 1995).Sporotrichosis has often been described among HIV patients, alcoholics, diabetics, and patients who used corticoids for a long period (Al-Tawfiq and Wools 1998; Silva-Vergara et al. 2012; Paixao et al. 2015). AIDS patients have a very poor prognosis because sporotrichosis spreads very easily. However, less commonly, immunocompetent individuals may have hematogenous spread and develop osteoarticular injuries (Almeida-Paes et al. 2014).
The most common clinical form in 80% of human cases is the lymphocutaneous form. Seven to 30 days after the traumatic inoculation, a nodule or ulcer develops at the inoculation site and adjacent lymphatic vessels (Bonifaz and Vazquez-Gonzalez 2013). The fixed form, which is more prevalent in Sporothrix globosa, consists of a single non-lymphatic nodule, which is limited and less progressive. This clinical manifestation is characterized by erythematous and occasionally ulcerated plaques, usually located on the face, neck, trunk, and legs. The lesions may undergo spontaneous remission but may relapse and persist for years if not treated (Fischman Gompertz et al. 2016).
The disseminated form is usually associated with some type of immunosuppression: HIV/AIDS, chemotherapy patients, advanced age, chronic alcoholism, diabetes, Cushing's syndrome, prolonged corticosteroid therapy, kidney diseases, and other conditions. After traumatic inoculation, the fungus spreads hematogenically (Al-Tawfiq and Wools 1998; Koeter and Jackson 2006; Orofino-Costa et al. 2010). Extracutaneous forms are also often associated with immunosuppression, but this relation is not mandatory (Kauffman et al. 2000, 2007). The extracutaneous form is common in immunocompromised patients such as diabetics, alcoholics, bone narrow transplant recipients, and patients with chronic lung disease or blood cancer. If Sporothrix spreads to the organs, the disease may present various symptoms such as sinusitis, meningitis, laryngitis, endophthalmitis, osteoarticular and pulmonary involvement, and fungemia (Silva-Vergara et al. 2012).
10.6
More on the topic ClinicalSigns:
- Haemobartonellosis (Eperythrozoonosis)
- Head Tilt and Nystagmus
- Alterations in the small intestinal microflora (Small intestinal bacterial overgrowth)
- SelectiveIgM Deficiency
- Small Ruminant Lentivirus Infections
- Steiner J.M. (ed.). Small Animal Gastroenterology. Schluetersche,2008. — 387 p., 2008
- Narcolepsy-Cataplexy
- Main Influences on Thyroid Function Tests
- Esophageal diverticula
- Causative Agents