Diagnosis
Vomiting that persists for more than seven days is considered chronic (Twedt 2010). If vomiting manifests in hematemesis then the patient should be triaged, hemoptysis, and coagulopathies are emergent conditions and can be confused with hematemesis from gastric ulceration.
Abdominal palpation will help determine if there is an abdominal mass or intestinal obstruction, but ultimately imaging is necessary. The time of vomiting relative to eating can be a clue as to the cause; vomiting more than 8 hours after eating indicates gastric outflow obstruction. Chronic gastritis, among other gastrointestinal diseases, is considered after exclusion of extra- gastric causes including pancreatitis, hypoadrenocorticism, renal failure, hepatobiliary diseases, and hyperthyroidism in the cat. A minimum database including hematology, biochemistry, urinalysis, and fecal flotation should be conducted. Peripheral eosinophilia could denote an eosinophilic gastritis caused by food allergy, and parasitism or hyperadrenocorticism, and pythiosis.Most lesions in chronic gastritis are thought to be restricted to the mucosa and submucosa and full thickness biopsies are not usually necessary (van der Gaag 1988). The benefit of endoscopy is that the gross assessment of the gastric mucosa is made (Figure 16.1) and focal lesions can be biop- sied. In cats, and a lesser extent dogs, full thickness gastric biopsies are superior due to the distribution of certain diseases, eosinophilic gastroenterocolitis, lymphoma and mast cell tumors infiltrate the submucosal and muscularis propria layers (Kleinschmidt et al. 2006; Kleinschmidt et al. 2010; Evans et al. 2006). Chronic gastritis is classified according to type - simple, hypertrophic, atrophic, or granulomatous - and the distribution of the infiltrate - superficial, diffuse, or follicular gastritis (van der Gaag 1988).
In addition the gastritis can also be classified according to the infiltrating inflammatory cell as follows: lymphoplasmacytic, eosinophilic, and granulomatous (Guilford and Strombeck 1996). Of vomiting dogs, 35% will have gastritis on endoscopy (van der Gaag 1988). The most common form of gastritis reported in vomiting dogs is superficial to diffuse gastritis, with atrophy and fibrosis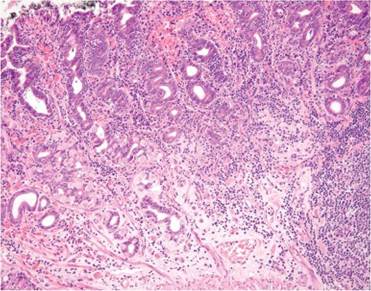
Figure 16.1 Gastric mucosa from a full thickness biopsy collected from the fundus of the stomach of a dog showing severe lymphoplasmacytic gastritis. Lymphocytes and plasma cells are present in severely increased numbers, diffusely and in aggregates, beneath epithelium and between glands, occasionally disrupting glandular architecture. Note mucous neck cell hyperplasia, increase in mucosal fibrous connective tissue, and nested, atrophic or loss of glands. (With permission, Dr Michelle Dennis, Ross University School of Veterinary Medicine).
occurring less commonly, 5% and 4% respectively (van der Gaag 1988). The most common type of gastric infiltrate in dogs with gastric pathology is lymphoplasmacytic (Lidbury, Suchodolski, and Steiner 2009).
Lymphoplasmacytic enteritis inflammatory bowel disease (IBD), manifests clinically with chronic vomiting, and is known to be associated with moderate to severe chronic antral gastritis (Garcia-Sancho et al. 2005). Thus IBD should be considered and investigated when this form of gastritis is diagnosed.
Confirming the presence of HLO includes a number of diagnostic tests in the cat or dog including, rapid urease test of biopsies, histopathology, cytobrush touch cytology smears using Gram or Diff quick stain, culture, polymerase chain reaction (PCR), fluorescent insitu hybridization (FISH) assay, and electron microscopy, with less invasive tests not being readily practical to small animal practice, that is, urea breath test, although this has shown to be helpful in predicting relapse (Neiger and Simpson 2000; Cornetta et al. 1998; Simpson et al. 1999; Lee et al. 1992; Neiger, Seiler, and Schmassmann 1999).
High gastrin concentrations are known to be associated with atrophic gastritis and neoplasia of gastric enterochromaffin cells like gastrinoma and in cases of Menetrier's disease. Gastrin concentrations are difficult to interpret as they are influenced by prior or current use of proton pump inhibitors, atrophic gastritis, hypochlorhydria, gastric outflow obstruction, small intestinal resection or short bowel syndrome, chronic renal- and liver failure, glucocorticoid excess, and hypercalcemia (Breitschwerdt et al. 1984). Acquired antral pyloric hypertrophy is diagnosed by means of ultrasound and endoscopy (Biller et al. 1994; Leib et al. 1993). Gastric infections with Pythium insidiosum should be considered as cause of gastric outflow obstruction in dogs from rural endemic areas.
More on the topic Diagnosis:
- Diagnosis
- Diagnosis
- Laboratory Diagnosis
- PATHOLOGY AND DIAGNOSIS
- Diagnosis
- Eosinophilic enteritis (EE)
- Ulcerations and Erosions
- Physical Examination
- Smith Mary C., Sherman David M.. Goat Medicine. 3rd edition. — Wiley-Blackwell,2023. — 976 p., 2023
- Physitis (Epiphysitis)