History of the disease
In 1885, after observing Leishmania organism for the first time, Cunningham stated that the organism was not a bacteria. Thirteen years later, a Russian military surgeon Peter Borovsky further found out that the organism was a protozoan which was also confirmed by Wright in 1903.
During that time, William Leishman and Charles Donovan described the agent responsible from VL. Leishman conducting his study in India observed enlargement of the spleen and fever in patients which he further observed the samples he took from the patients under the microscope using Romanowsky method for staining and stated that it was not like anything he had seen before [13]. Finally, in 1942, female phlebotomine sandflies had enough evidence to be accepted as the main vector for CL and VL due to the fact that clinical conditions observed following a sandfly bite described as histiocytoses [14]. In terms of changing face of diagnosis of leishmaniasis, starting from the microscopical identification of the agents, medical technologies have progressed in time further into PCR-based DNA sequencing methods for determination of specific species.L. donovani was the first identified Leishmania species taking its name from William Leishman and Charles Donovan which was given by Ross in order to give credit to their studies [15].
Despite being a neglected tropical disease, our knowledge about the disease has been increasing continuously. Case reports involving uncommon laryngeal leishmaniasis- and HIV-infected individuals showing leishmaniasis effects such as skin lesions and nodules have shown that leishmaniasis can occur again even after treatment hinting to the incubation period of parasite (Figure 1) [16, 17].
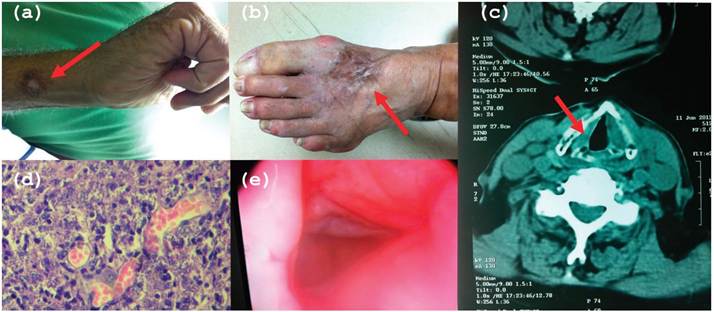
Figure 1.
A rare case of treated laryngeal ML which Originatedfrom a previous CL of hands and feet.
Isolated agent is L. infantum in this 81-year-old male patient resident in Adana, Turkey, a subtropical area. (a) CL lesions on a patients hand on his first application to clinic. (b) CL lesions on patients foot on his first application to clinic. (c) BT of neck showing papillomatous push elongating into ventricles. (d) Histological examination of laryngeal biopsy specimen (May-Grunwald-Giemsa staining; original magnification, ?1000) showing intracellular amastigotes of Leishmania species and histiocytes with vacuolated cytoplasm and corpuscles inside. (e) Laryngoscopic examination showing lesions with edema and erythema due to ML. Reprinted from [16].Treatment of leishmaniasis started with the use of pentavalent antimonials in the 1940s. Parasite gaining resistance and high level of toxicity for these drugs made it necessary to find an alternative. Amphotericin B is an alternative drug that has been in use since 1980. The main action mechanism of amphotericin B is to interfere with the membrane lipids and cause disruption. The length of the therapy changes between 15 and 45 days for different cases, whereas dosage can vary. Combinatorial use of this drug with some other drugs has shown great increase in the effectiveness of treatment.
3.
More on the topic History of the disease:
- Diagnosis
- THE PAEDIATRIC CONSULTATION AND CLINICAL CONSIDERATIONS
- Medical Record
- Introduction
- Surveillance
- Smith Bradford P., Van Metre David C., Pusterla Nicola (eds.). Large Animal Internal Medicine. Part 2. 6th edition. — Elsevier,2020. — 2279 p., 2020
- NON-INFECTIOUS DISEASE
- Intestinal obstruction - intestinal foreign bodies, intussusception, and intestinal torsion
- Interpretation of the Findings
- Nutritional Diseases