Hyperketonemia in Dairy Cattle (Ketosis)
Jessica A.A. McArt • Daryl Nydam
Pathophysiology
Most dairy cows visit a state of energy deficit, often termed negative energy balance (NEB), as they transition from late gestation to early lactation.
This imbalance in energy is the result of both an increase in energy requirements—more than twice as high when compared with prepartum levels1—and inadequate DMI. The increase in energy demand is due to lactogenesis, which is dependent on available glucose concentrations from gluconeogenesis in the liver.2 Ruminal fermentation provides the majority of substrates for hepatic gluconeogenesis through production of volatile fatty acids (VFA), the most abundant of which are acetic acid, propionic acid, and butyric acid. Propionic acid is absorbed by the liver via portal circulation and serves as the primary metabolite for gluconeogenesis. Acetic acid is used mainly in the liver as a major source of acetyl CoA to generate ATP, and butyric acid is absorbed directly from the rumen as the ketone β-hydroxybutyrate (BHB), which can be used by multiple tissues for energy production. Several factors (e.g., nutrition, ionophore use, DMI) determine the amount and proportion of VFA produced, and when the cow's requirement for energy exceeds her productive capacity, NEB ensues. At the individual animal level, there are several metabolic adaptations to manage NEB, which include mobilization of nonesterified fatty acids (NEFA) from body fat reserves and glucose sparing for lactogenesis. However, some animals will experience excessive NEB, and it is this excess that is associated with negative downstream outcomes such as increased risk of disease development and decreases in both milk production and reproductive performance.3-5 As some degree of NEB postpartum is physiologically normal, it is its depth, duration, and timing that influence the cow's health and performance. The metabolites NEFA and BHB are used as markers of NEB due to the relationship among energy demands, energy reserves, and the metabolic association between NEFA and BHB. Fig. 41.25 is a graphic representation of the association between these factors, which can result in excessive concentrations of BHB and the syndrome of hyperketonemia.To adapt to this increase in energy demands, glycerol and NEFA are released from adipose tissue in response to hormonal cues, such as glucagon, corticosteroids, adrenocorticotropic hormone (ACTH), and catecholamines. Insulin is the only hormone that will act to inhibit lipolysis and therefore decrease the amount of NEFA released from adipose tissue. Early in the postpartum period, there is both a decrease in insulin production and perhaps a transient state of insulin resistance.1 This spares glucose for lactogenesis by decreasing glucose utilization in insulin-sensitive tissues and allowing continued lipolysis even when insulin concentrations increase, though the mechanistic pathways in postpartum dairy cows remain complicated.6
■ TABLE 41.8
Diagnosing Acute and Chronic Macromineral Insufficiency or Imbalance in Ruminants
The tissue needed to ascertain acute problems is intended to guide diagnosis of the initial cause of recumbency in downer cows. All fluid concentrations are in mg/dL. “Subclinical” indicates no readily apparent outward signs of illness. “Clinical” will generally result in a “down” cow.
| Mineral | Tissues to Use | Normal | Subclinical | Clinical |
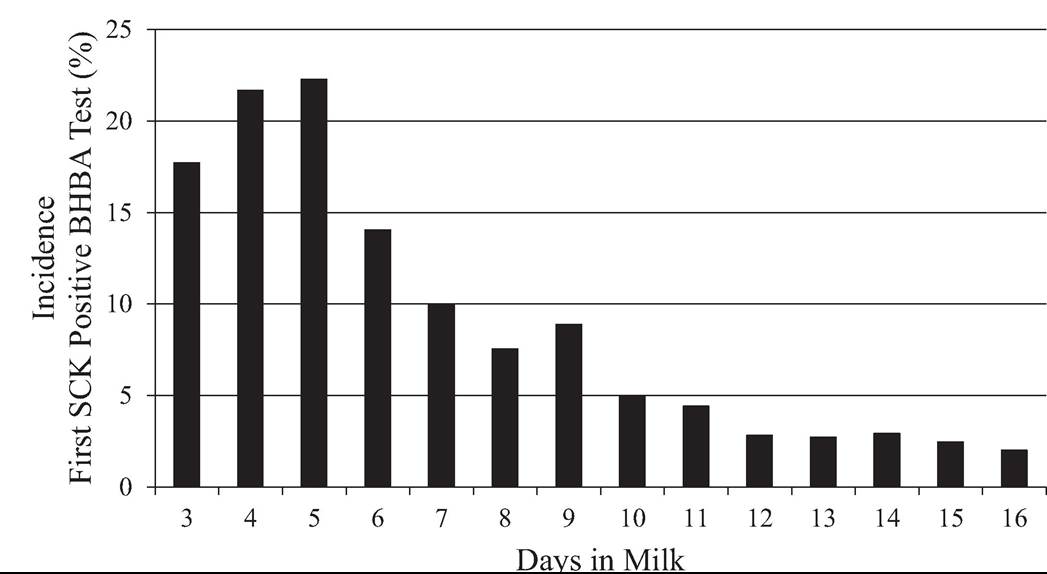
| Ca (Acute) | Serum | 8.0-10.5 | 5.5-7.5 | suggests a more severe hyperketonemia compared with cows that do not show clinical signs. Recent research has provided solid and repetitive evidence of quantitative blood BHB concentration cut-points that result in increased risks of subsequent disease development and production loss. This cut-point falls somewhere around 1.2 to 1.4 mmol/L depending on the desired sensitivity and specificity4,5,11; a lower cut-point results in a higher test sensitivity and lower specificity, and a higher cut-point results in a lower sensitivity and higher specificity. Thus, subclinical ketosis technically includes those cows with concentrations of BHB above 1.2 mmol/L that do not have clinical signs, and cows with clinical signs would, by definition, have clinical ketosis irrespective of what their blood concentration is (though it is often above 2.5 to 3.0 mmol/L). Hyperketonemia includes both of these categories and is the preferred term, encompassing all cows with elevated BHB regardless of expression of clinical signs. Type 1 and type 2 ketosis are terms loosely borrowed from human medicine and diabetes literature. They have limited utility in aiding our understanding of hyperketonemia in modern dairy cows or in how we prevent or treat the condition. Clinical Signs and Differential Diagnoses Of hyperketonemic cows, 85% to 95% have blood BHB in the 1.2 to 2.9 mmol/L range and show no aberrant clinical signs4,12,13; thus, we cannot detect most cases of mild or moderate hyperketonemia during a physical examination without additional diagnostic testing. Clinical signs expressed by cows with severe hyperketonemia are vague and similar to those seen with other early lactation diseases, including a loss of appetite, a decrease in milk production, and a more profound weight loss than normally seen during this period of lactation. It is important to note that the severity of hyperketonemia is not highly associated with clinical signs in that many severely hyperketonemic animals do not show clinical signs. On physical examination, hyperketonemic animals (without concurrent disease) will have normal vital signs and may have decreased rumination frequency with more severe disease. The odor of ketones may be detected in the breath of some hyperketonemic cows, and many will have hyperketonuria. It is well established that hyperketonemia increases the risk of additional early lactation diseases such as metritis and displaced aboma- 41213sum4 ; thus, a complete physical examination is necessary to identify or rule out other concurrent diseases. In a very small percentage of severely hyperketonemic cows, an acute onset of bizarre neurologic signs will be evident, which can include excessive licking, flank-sucking, bellowing, circling, head pressing, and apparent blindness, and may progress to tremors and tetany. These cows are classified as having nervous ketosis and may be aggressive toward people or their surroundings, so care for personal safety is heightened during examination. Differential diagnoses for nervous ketosis include rabies, listeriosis, hypomagnesemia, and acute lead poisoning. Epidemiology Numerous studies have described the detrimental association of hyperketonemia with additional postpartum diseases, particularly metritis and displaced abomasum,11-14 and culling in early lactation.13,15,16 From an epidemiologic standpoint, it is important to know which disease occurs first to attribute the development of the secondary disease to the primary one. In most of the aforementioned studies, good effort has been made to record the temporal association of these diseases, and in the vast majority of cases, hyperketonemia has been diagnosed before metritis and displaced abomasum, such that 70% of metritis cases and 88% of displaced abomasum cases can be attributed to hyperketonemia.17 This increased risk of disease, culling, and poor production rises not only as the severity of hyperketonemia increases, such that a cow with a BHB of 3.5 mmol/L is much more likely to develop a displaced abomasum as a cow with a BHB of 1.2 mmol/L, but also as the DIM at first diagnosis decreases (i.e., a cow first hyperketonemic at 3 DIM is much more likely to develop a displaced abomasum than a cow first hyperketonemic at 8 DIM).13,14 Peak incidence and prevalence of hyperketonemia (diagnosed in this case as a BHB concentration of 1.2 to 2.9 mmol/L) were found to occur at 5 DIM (Fig. 41.26) after intensive, three-times-per-week monitoring of 1717 cows on four large TMR-fed freestall dairies in New York and Wisconsin, United States.13 A similar peak in prevalence of hyperketonemia (diagnosed as a BHB concentration of ≥1.2 mmol/L) at 1 week postpartum was reported by Duffield and colleagues18 using data from 1010 cows on mostly component-fed tiestall dairies in southwest Ontario, Canada. As the median time to resolution of hyperketonemia was reported to be 5 days,13 farms that test less frequently than twice per week will underestimate the true incidence.
FIG. 41.26 Histogram of incidence of subclinical ketosis (SCK) in 1717 Holstein dairy cows undergoing repeated testing for SCK from 3 to 16 DIM. A positive test was defined as a blood BHBA concentration of 1.2 to 2.9 mmol/L. (Adapted from McArt JAA, Nydam DV, Oetzel GR: Epidemiology of sub-clinical ketosis in early lactation dairy cattle. J Dairy Sci 95:5056-5066, 2012.) Two important measurements that help evaluate the frequency of a disease in a farm population are incidence risk and prevalence. Incidence risk is estimated by dividing the number of cows affected with a new case by the total number of cows that have gone through this time period (i.e., the number of cows that develop a disease at any time during a given period, among those who are at risk). For determining the incidence of hyperketonemia, a cow is no longer at risk as a new case once she has been diagnosed positive. When estimating incidence, it is necessary to follow a group of cows throughout the entire time period of interest, and testing must be completed frequently enough to ensure that all cows that develop disease will be correctly identified. For example, if a disease typically lasts 5 days, all cows at risk must be tested at least two times per week. As an example, if 15 cows within a group of 50 at-risk cows that were monitored between 3 and 16 days in milk (DIM) developed hyperketonemia for the first time sometime between 3 and 16 DIM, the incidence risk of hyperketonemia during that time period would be 30% (15/50). Prevalence is a snapshot of the amount of a disease existing in a herd at a single point in time; it is determined by one test and is thus easier to estimate than incidence. Prevalence is calculated by dividing the number of disease-positive cows by the total number of cows sampled at that point in time. For example, if 20 cows were tested on a single day and three cows were hyperketonemic, the prevalence would be 15% (3/20). At the herd level, the recommendation is to test at least 15 to 20 cows in the appropriate DIM range each time a prevalence test is conducted. The recommended number of cows to test depends on the number of cows at risk, the expected herd prevalence, and the user's acceptance of the precision of the estimate and the confidence interval around the estimate. For example, if there are 50 fresh cows at risk for hyperketonemia (i.e., between 3 and 16 DIM) and you expect the prevalence to be 15%, sampling 20 cows will allow you to be 90% confident that the prevalence you obtain is ±10% of the true herd prevalence. This is a relatively small number of animals to test, but it is only useful for determining whether a herd has a very low or very high prevalence of the disease. More cows should be tested in order to more confidently estimate the true herd prevalence. For example, sampling 40 cows in the above scenario will allow you to be 95% confident that the prevalence you obtain is ±5% of the true herd prevalence. Knowing a herd's estimated incidence of hyperketonemia is more useful than knowing the prevalence because the best strategy for testing and treating individual cows for hyperke- tonemia depends on the herd incidence. However, a direct determination of the herd incidence is practically challenging because it requires repeated testing of individual cows frequently enough so that all cows that develop hyperketonemia are identified. Work by McArt and colleagues13 showed that the average duration of hyperketonemia was 5 days; thus, cows must be sampled a minimum of twice per week in order to appropriately estimate incidence. A reasonable alternative is to conduct a simple cross-sectional sample (testing herd prevalence) and then estimate the herd incidence from the herd prevalence. Fortunately, the incidence of hyperketonemia has 13 18 been consistently reported to be about twice its prevalence.13,18 For example, if 100 early lactation cows from a herd were tested and 15 of these cows had blood BHB greater than or equal to 1.2 mmol/L, the herd prevalence would be 15% and the estimated herd incidence would be 30%. Within-herd incidence of postpartum hyperketonemia appears to range between 25% and 60% with an average of approximately 45%; across all herds in these studies, 47% of cows tested positive at least once. The results from Duffield and colleagues,13 however, tested cows only once weekly and thus likely underestimated the true incidence. Approximately 20% of sampled cows have elevated BHB in the first 2 weeks postpartum, with within-herd prevalence ranging from 0% to 71%.4,14 The prevalence of herds in which more than 15% of sampled cows had increased postpartum BHB concentrations of greater than or equal to 1.2 mmol/L was 40%.4 Chapinal and colleagues19 reported that the prevalence of herds in which more than 25% of sampled cows had increased postpartum BHB concentrations of greater than or equal to 1.4 mmol/L was 15% in 55 herds in the United States and Canada tested within a week postpartum. These two studies also reported on within-herd alarm thresholds and subsequent outcomes. Chapinal and colleagues19 reported reduced milk yield based on production at first Dairy Herd Improvement test of 4.4 kg per cow per day when greater than or equal to 15% of sampled animals had prepartum BHB concentrations greater than or equal to 0.8 mmol/L. In addition, herds where greater than or equal to 25% of sampled animals had postpartum BHB concentrations greater than or equal to 1.4 mmol/L had increased odds of DA. Ospina e and colleagues4 found that herds in which greater than 15% of sampled animals had postpartum BHB concentrations greater than or equal to 1.2 mmol/L, the risk of cows with DA and clinical ketosis was higher and the herds had an increased time to pregnancy and produced less milk compared with herds with fewer animals above the threshold. Results from these studies suggest that herds with greater than or equal to 15% to 25% of sampled animals having increased prepartum or postpartum NEFA or BHB concentrations may have more difficulty with postpartum disease, poorer reproduction, and lower milk production than herds with a lower proportion of positive animals. Economic Impact For cows that develop any transition cow disease, the total cost of that disease can be divided between component costs and attributable costs, where the component costs are the sum of the direct and indirect costs of that particular disease and the attributable costs include the increased risk of developing another related disease. The direct costs of a disease include labor and veterinary services associated with diagnosis and treatment, therapeutic interventions, and discarded milk required for these interventions. Indirect costs consist of future losses such as milk production, premature culling of the cow as a result of the disease, and negative impact on future reproduction. While most people readily realize the direct costs associated with a disease, interestingly, these make up a relatively small part of the total cost of a disease. For hyperketonemia, the average component cost per case is estimated to be $117.17 Interestingly, the direct costs associated with the disease are only approximately 6% of the total cost, with the remaining 94% of associated costs being indirect, largely future reproductive and milk production losses. When including the costs of other diseases attributable to hyperketonemia (i.e., metritis and displaced abomasum), the total cost per case is almost $290. With herd early-lactation hyperketonemia incidences averaging 40%,13,18 annual costs due to hyperketonemia are not trivial. Necropsy Findings Mortality due to hyperketonemia is uncommon unless the disease is severe in nature with an associated hepatic lipidosis, which is often the only pathologic finding during a gross necropsy examination. CLINICAL PATHOLOGY AND DIAGNOSTIC TOOLS. The diagnostic hallmark of hyperketonemia is, as the name suggests, elevated blood ketone bodies. As BHB is the most stable ketone body in blood, its concentration is the accepted gold standard method for diagnosis of hyperketonemia. Numerous studies have assessed clinical disease incidence, culling risk, and subsequent milk production associated with various BHB cut-points to optimize use of a threshold for diagnosis of hyperketonemia, and widely used cut-points vary from 1.2 and 1.4 mmol/L.12,14,20 As mentioned earlier, the choice of which cut-point to use depends on the user's testing purpose and desire to maximize the resulting sensitivity or specificity of the test. Recent advances in portable technology over the past decade have produced vast improvements in on-farm hyperketonemia detection with handheld point-of-care BHB meters. These can be used with whole blood, serum, or plasma and allow for an inexpensive, rapid, and accurate method for both individual cow hyperketonemia detection and herd-level disease monitoring.21,22 Although inexpensive, urine ketone tests, while highly specific, suffer from poor sensitivity.23 Combined with a typical success rate of 50% when attempting to induce urination in a given cow, urine ketone tests lag behind handheld BHB meters in clinical utility for use in individual cow identification of hyperketonemia. Tests for milk ketones have a similar poor sensitivity, and given a comparable cost to blood BHB testing are an inferior test at the individual cow level. The poor sensitivity of urine and milk ketone tests precludes their use as a herd-level hyperketonemia monitoring tool. Additional testing is usually unnecessary for diagnosis of hyperketonemia and rarely improves prognostic decision making, even in cases with accompanying hepatic lipidosis. Treatment and Prognosis Although hyperketonemia has been a commonly encountered disease for decades, few randomized, controlled studies have been conducting that assess the efficacy of frequently administered treatments.24 The goal of such treatments are to increase the availability of glucose, whether directly administered or produced by the cow, to decrease adipose tissue mobilization and increase uptake of glucose by cells. Administration of a glucose precursor, given as a drench, provides a source for gluconeogenesis and creates an insulin surge to facilitate glucose transport into cells. Food-grade propylene glycol is the most common product used for this purpose, and treatment with a multiday course has been shown to increase the speed of hyperketonemia resolution, reduce the risk of subsequent disease, and increase milk production.25,26 Propylene glycol acts by increasing blood glucose concentrations through its conversion to propionate, both in the rumen and through hepatic metabolism of propanol, as well as by decreasing peripheral tissue glucose demand induced by circulating blood levels of propylene glycol and propanol.27 A dose of 310 g (300 mL) once a day for 3 to 5 days is recommended; oral drenching is preferred over mixing in the feed to induce an insulin spike and for palatability reasons. Although glycerol can be administered as a glucose precursor and is highly metabolized in the rumen, no randomized field trials have been conducted to assess its effectiveness. A small study comparing propylene glycol with glycerol treatment in aboma- sally cannulated cows showed that glycerol had no benefit over propylene glycol treatment unless administered directly into the abomasum, which is not feasible in a clinical setting.28 The importance of administering these glucose precursors as a drench rather than mixing with the feed is due to the desire of the resulting insulin surge, which is not seen when propylene glycol is mixed with the ration. A review of multiple studies feeding propylene glycol in the ration concluded that it had no impact on milk production when administered in this way.29 Current trials are under way to investigate the effect of new dried propylene glycol and glycerin products fed continuously via the ration during the transition period. Propionate has been implicated as a major player in hepatic oxidation theory, the concept that feed intake is regulated by oxidation of fuels (fatty acids, propionate, lactate, and amino acids) in the liver, with higher rate of fuel oxidation suppressing feed intake.30 Although administration of propylene glycol and other glucose precursors increases propionate availability, no studies have shown that this treatment suppresses feed intake.29,31 However, most field trials with the statistical power needed to appropriately answer this question cannot adequately measure DMI on an individual cow basis; thus, most studies reporting a lack of association with propionate and DMI are underpowered for this analysis. Interestingly, the success of historical therapy with an intravenous injection of glucose (in the form of dextrose) has never been assessed in a large, randomized field trial in the treatment of hyperketonemia. A recent small study showed that intravenous administration of 500 mL of 50% glucose was effective in reducing blood BHB concentrations in hyperketonemic cows for approximately 4 hours; the transient hyperglycemia from glucose administration lasted for 2 hours. However, the most effective treatment for a prolonged decrease of blood BHB concentration was seen when intravenous glucose and oral propylene glycol were given in combination.31 There is some debate regarding the total grams of administered glucose, with some clinicians preferring 250 mL of a 50% glucose solution over 500 mL due to the potential of a resulting insulin-induced hypophosphatemia and additional electrolyte disturbances on excretion of extra glucose by the kidney. However, no hypophosphatemia or other mineral or electrolyte disturbances were seen after 3 days of treatment with 500 mL of 50% glucose.31 It is also debated whether a continuous intravenous infusion of 2.5% or 5% glucose over a 24-hour period is preferred over multiple 50% glucose administrations. Regardless of the inability to perform a constant infusion in a commercial herd setting, there is no evidence that one infusion method is superior over the other in the treatment of hyperketonemia. Glucocorticoids have been used for decades to treat hyperketonemia given their action in stimulating gluconeogenesis and providing glucose precursors; however, few studies have scientifically supported the use of glucocorticoids in the treatment of hyperketonemia. Although glucocorticoids may reduce blood BHB concentrations in the short term, particularly for mild hyperketonemia cases, their use from a subsequent disease and production standpoint has rarely been assessed. Data from a recent large field trial suggest even one dose of dexamethasone (20 mg) at diagnosis of hyperketonemia may be detrimental to cows with BHB greater than 3.2 mmol/L, and that a one-dose treatment had no positive effects on health or production outcomes at any severity level.32 Given the lack of benefits of glucocorticoids on disease incidence or milk production in mild cases and the potential detrimental effects in more severe hyperketonemia cases, the routine use of glucocorticoids is not recommended for the treatment of hyperketonemia. Insulin has been used as an adjust therapy for hyperketo- nemia in conjunction with glucose administration. However, there is limited evidence supporting its use for treatment of hyperketonemia, and the high cost of most commercial products prevents their widespread use and further investigation. Insulin suppresses adipose tissue mobilization, increases uptake of glucose by tissues, and stimulates hepatic glycolysis. Its use with glucose over several days of treatment has been shown to reduce BHB, fatty acids, and liver triglycerides; however, no studies have looked at economically important outcomes from treatment to ascertain if insulin impacts subsequent disease incidence or milk production. Recent work suggests one dose (200 IU) of glargine insulin increases milk yield in older parity hyperketonemic cows with concurrent hypoglycemia, although it was also found to decrease milk yield in the same age group of cows that were euglycemic. Given the cost and equivocal results on health and production outcomes, the routine use of insulin for the treatment of hyperketonemia is not supported. Vitamin B 12 has been used in the treatment of hyperketonemia, usually in the chemically synthesized form, cyanocobalamin, and often in combination with butaphosphan (Catosal, Bayer, Shawnee, Kan.). As a vitamin B12-dependent enzyme, methymalonyl-coenzyme A mutase, plays an important role in the transfer of propionate into the TCA cycle, it is thought that increasing the activity of this enzyme through administration of vitamin B12 may increase gluconeogenesis. The few studies that have analyzed the effect of vitamin B12 have found that it increases ruminations in the few days after treatment and increases the cure risk in hyperketonemic cows with concurrent hypoglycemia over that of nontreated hyperketo- nemic cows.33,34 Given the low cost of vitamin B12, it is often administered as an adjunctive treatment with propylene glycol at 2 to 5 mg per day, although without scientific proof of effectiveness. The prognosis for resolution of mild hyperketonemia is excellent depending on subsequent disease development. Cows developing hyperketonemia in the first week of lactation, as well cows with more severe hyperketonemia, are at a higher risk of negative health events and poorer milk production in early lactation. Thus, both the timing of hyperketonemia development and severity can be used as prognostic indicators of subsequent disease risk.13,32 With appropriate identification and treatment, the majority of hyperketonemic cows resolve their disease within 1 week and continue on to productive lactations. The prognoses of hyperketonemic cows that develop additional early-lactation diseases such as metritis or displaced abomasa depend on their response to treatment for the respective associated disease. Cows with accompanying severe hepatic lipidosis have a much poorer prognosis as constant and repeated nursing care is important in addition to the treatments discussed earlier, which takes considerable time and financial resources. Herd-Level Prevention and Control Whereas previously discussed ketone tests have great use as tools for diagnosis of hyperketonemia in individual animals, they can also be incorporated into a program for herd-level monitoring in order to assist with management decisions. It is important to note that the sensitivity and specificity of different tests can have a large impact on individual test results and, as a consequence, herd diagnosis and treatment. The probability of correctly identifying a herd as positive (i.e., having a prevalence of hyperketonemia above a certain threshold) decreases when a test with low sensitivity is used.35 For these reasons, use of handheld blood BHB meters are suggested for herd-level monitoring. As noted earlier, herds with a high prevalence of hyperketo- nemia are more likely to have a higher incidence of postpartum disease, poorer reproduction, and lower milk production. Research completed in over 150 herds in the United States and Canada suggests that this association between herd hyper- ketonemia prevalence and disease and production outcomes occurs when greater than or equal to 15% to 25% of animals have elevated postpartum blood BHB concentrations.15,19 Ospina and colleagues15 found that 40% of the 100 herds tested were above the herd alarm level. Unfortunately, hyperketonemia is an issue on many herds, and additional studies have found the incidence and prevalence of hyperketonemia to be quite high across herds in the United States, Canada, and Europe. On a herd-level treatment basis, when the incidence of hyperketonemia rises above 25%, almost any testing and treatment strategy for hyperketonemia is economically beneficial. If herdlevel incidence exceeds 50%, blanket treatment of all fresh cows with propylene glycol is recommended, beginning no earlier than 3 days in milk.17 The delay of blanket treatment until a few days into lactation is important, as most cows are hyperglycemic in the immediate postpartum period, and administrations of propylene glycol, a glucose precursor, may exacerbate hyperglycemia and induce insulin dysregulation. If blanket treatment of all fresh cows is implemented, herd-level assessment of transition cow management, discussed later, is warranted, with repeated testing of fresh cows to monitor hyperketonemia prevalence at least monthly. The goal of herd-level hyperketonemia management strategies and monitoring programs are to keep the prevalence of hyperketonemia below 15%.35 Traditionally, nutritional management of dairy cows during the far-off dry period (i.e., approximately 60 to 30 days before calving) has received little attention, but it is a key area for hyperketonemia control. Indeed, many aspects of nutritional management (e.g., mineral nutrition beyond meeting basic nutrient requirements) appear to be less important during the far-off period compared with the close-up period. However, several studies36-39 suggest that overfeeding cows beginning during this period leads to lower postpartum DMI, increased mobilization of body tissue, increased circulating concentrations of NEFA and BHB, and increased risk for metabolic disorders and poorer productive and reproductive performance. The recommended target diet formulation is to meet 110% to 120% of energy requirements during this period and metabolizable protein supply for Holsteins of over 1200 g/day. During the far-off period, macromineral considerations such as potassium are not of great concern; thus, a wider array of forages and feeds are acceptable to form the basis of diets. As described earlier, controlling energy intake of close-up cows so that they meet, but do not dramatically exceed, their energy requirements during this period is a critical target. As has been well documented previously and supported by recent research,4,15,35 energy intake below requirements as reflected by elevated NEFA concentrations during the close-up period is associated with increased incidence of postpartum metabolic disorders, lower milk production, and poorer reproductive performance. The recommended target energy intake of cows during the close-up period is 110% to 130% of energy requirements. For Holsteins, this is in the range of 16 to 18 Mcal/day of NEL. As a starting point, formulate the close-up diet at approximately 1.45 Mcal/kg of NEL if the group is a comingled cow/heifer group and approximately 1.38 to 1.40 Mcal/kg of NEL if the group is composed of mature animals and DMI is high. These energy densities are adjusted on the basis of actual DMI of cows on farms to achieve the overall targets for energy intake during the close-up period described earlier. Metabolizable protein supplies of at least 1200 to 1300 g/day for cows during the close-up period should be targeted.40 Given that lower-energy diets fed during the close-up period as described earlier typically contain limited amounts of rapidly fermentable carbohydrate (16% to 18% starch), microbial protein synthesis is limited and diets generally contain 1 to 2 kg of ruminally undegradable protein sources in order to meet the metabolizable protein recommendation outlined earlier. Furthermore, research generally supports formulation of close-up rations with methionine and lysine at levels similar to those used for lactating cows. To prevent hyperketonemia and other metabolic disorders of transition cows, it is important that neither protein nor energy are limited. This must be done while avoiding excessive energy intake. Other management factors are certainly involved in the observed differences between farms and cows and could lead to an increased risk for hyperketonemia early in lactation. These include inadequate cow comfort, high stocking density (e.g., >80% in the close-up and fresh group), unnecessary pen moves, inadequate heat abatement, and limited access to water. Having high-quality feed (silage high in butyric acid has been repeatedly found to cause hyperketonemia, both through a reduction in DMI and a direct conversion of butyrate to BHB in the rumen) available at least 23 hours of the day, as well as management programs in place for the prevention of infectious diseases such as mastitis and uterine infection, aid in the decrease of the risk for this metabolic derailment. Mature cows, cows that had a difficult calving, and overconditioned cows are generally at an increased risk to develop hyperketonemia at the beginning of lactation.
More on the topic Hyperketonemia in Dairy Cattle (Ketosis):
-
Veterinarian -
|