Trauma to the Brain and Cranial Nerves
Robert J. MacKay
Because of their flighty temperaments, fast gaits, and relatively thin calvaria, horses suffer head trauma more often than do other livestock and have a higher rate of neurologic sequelae of such trauma (i.e., traumatic brain injury).
Head injuries to horses occur from blows to the frontal-parietal area from running into stationary objects or being kicked by other horses, as well as from impact to the occipital protuberance (poll) or temporal areas after flipping over backward during handling or restraint accidents.1 Specific cranial nerves may also be injured on the outside of the skull by focal trauma. In the special case of THO, fractures of the petrosal bone can occur suddenly without any external trauma. THO is covered in a separate section. Penetration by missiles, most often bullets, is also a cause of neurotrauma in horses. Missile head injury is not be covered in this section, but a review of the subject is available elsewhere.2Frontal/Parietal Trauma
Blows to the front of the head over the dome of the calvaria directly injure the cerebral cortex adjacent to the point of impact.3 Brain injuries are most severe when the overlying bone is fractured and pushed inward or if hemorrhage occurs around or within the brain. Because of the violent distortions and movements of the cerebral hemispheres in relation to the impact, additional cortical injuries may occur diametrically opposite the point of collision (contrecoup) and caudally adjacent to the tentorium cerebelli. With the development of the secondary phase of cerebral injury and edema, the enlarging cerebral hemispheres herniate under the falx cerebri (asymmetric injury) or tentorium cerebelli, or both, to compress other parts of the brain. Horses may recover from the acute effects of calvarial fracture only to suffer recurrent seizures later.
Horses that collide at speed with fixed objects are at risk for both head trauma and spinal cord injury.4Impact to the Poll and Temporal Areas
When a horse flips over backward, the point of contact is either the poll or the side of the skull.5-14 Of 34 horses with neurologic signs due to head trauma, 15 were injured by flipping over backwards.15 Nine of these horses were younger than 1 year. The force of impact is absorbed by the poll, the zygomatic arch, or both and transmitted around the skull to the petrosal bones. Presumably because of the asymmetry of impact, only one side is usually injured. This may be either the upper or lower (i.e., impacted) side. There is hemorrhage into the middle and inner ear with or without fracture through the petrosal bone. The vestibulocochlear end organs in the inner ear are vulnerable to injury by both hemorrhage and the lacerating
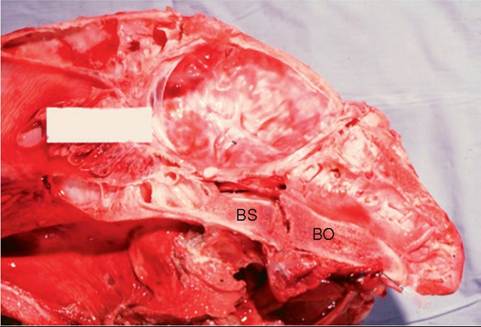
FIG. 35.9 Sagittal section of the skull of a 2-year-old colt that flipped backward during handling and suffered multiple skull fractures. Note separation/fracture in the region of the synchondrosis between the basioccipital (BO) and basisphenoid (BS) bones and hemorrhage in the region of the attachment of rectus capitis ventralis major.
effects of fracture. In the latter case, the facial nerve may be damaged as it courses through the facial canal within the petrosal bone. When the point of impact is centered on the poll, the basilar bones under the brainstem are subject to fracture and separation (Fig. 35.9). The basioccipital and basisphenoidal bones are pulled apart at their synchondrosis connection, at least in part by the strong distracting force of the rectus capitis ventralis muscles. Fragments of bone from the basisphenoid may be displaced ventrally and caudally by muscular attach- ments.14 Because the synchondrosis is beneath the midbrain and flanked on each side by the foramina lacera and guttural pouches, basilar fractures are clinically serious.
There may be life-threatening arterial hemorrhage between or into the guttural pouches; injury to cranial nerves IX (glossopharyngeal), X (vagus), XI (accessory), and the mandibular branch of V (trigeminal) as they pass through the foramen lacerum; direct laceration and contusion of the midbrain and adjacent parts of the brainstem; or a combination of these. Because the connection between the basilar bones ossifies and fuses by 2 to 5 years of age, this type of injury is probably more likely to occur in young horses. In the most serious cases, fracture lines extend laterally and dorsally through the squamous temporal and occipital bones or rostrally through the sphenoidal bones (see next section).Other Cranial Nerve Injuries
The optic nerve of one or both eyes can be stretched and damaged within the optic canals by the violent to-and-fro gyrations of the brain after impact to the head12,16 and by fractures through the optic canals. Sphenoidal bone fractures also may involve cranial nerves III (oculomotor), IV (trochlear), and VI (abducens) or the ophthalmic and maxillary branches of cranial nerve V as they pass to the orbital foramen and foramen rotundum. Injury to the facial nerve proximal to the vertical ramus of the mandible causes full facial paresis. Proximal facial nerve trauma is usually caused by fractures of the petrosal bone, vertical ramus of the mandible, or stylohyoid bone or by fracture of the paracondylar process related to pulling back in a tied horse.17 Distal facial nerve damage is usually due to direct injury from a blow, lateral recumbency, or strangulation by a tight-fitting halter. Cattle whose heads are clamped in the head-catch on stanchions may present with “stanchion head” or ptosis and drooping ears caused by bilateral neurapraxia of the auriculopalpebral branches of the facial nerves. The nerve or its branches are often damaged as they cross the mandible or zygomatic arch. Facial paresis after recumbency during general anesthesia is common and usually involves only the nose, lips, or both.
When a horse pitches headfirst into the ground while traveling at speed, it is possible for components of a fractured atlas to be driven rostrally around the occipital condyles, where they may traumatize cranial nerve XII (hypoglossal) as it exits the hypoglossal foramen.Skull fractures occur in cattle from blows to the top of the calvaria.18 Most skull fractures are located in the center of the frontal bones, where the internal and external plates of the frontal sinus are fused into a single-layer dorsal wall of the cranial vault. This position can be located on the skull as the imaginary cross formed by intersecting lines drawn between the medial canthus of the eye and the horn of the opposite side. Injuries in this area compress the frontal and parietal lobes of the cerebral cortex. The pressure changes result in loss of sensorium, sensory deficits, blindness contralaterally, or convulsions.
In young goats and horned sheep younger than 4 to 6 months of age, the calvaria can be inadvertently opened by removal of excessive bone during disbudding or dehorning. In goats, cerebrocortical burns can occur from overapplication of a hot iron or caustic dehorning paste. Cortical necrosis caused by bacterial infections after dehorning of calves has also been described.
■ Clinical Signs Epistaxis is common after a blow to the head of severity sufficient to cause neurologic signs.5,9 After frontal/parietal or poll trauma, blood may flow from either or both nostrils and is typically dark (venous) and of low to moderate volume. With poll trauma, epistaxis may be bilateral, copious, and occasionally bright red, and may also issue from the mouth.14 In such cases, the hemorrhage is from one (usually) or both guttural pouches and originates from adjacent veins or arteries.19 If the tympanum is perforated, blood may flow in addition from the external ear. Profuse hemorrhage into the retropharyngeal area may cause obvious swelling behind the vertical ramus of the mandible and inspiratory dyspnea, which can be life-threatening.
Respiratory distress may also be associated with a poorly understood syndrome of noncar- diogenic pulmonary edema that is reported to occur after serious head injury. Head trauma in humans is often complicated by systemic arterial hypotension. The cause is not completely understood but may be explained in part by brain-heart syndrome, in which myocardial damage is inflicted by the reflex actions of sympathetic nerves.Immediately after impact to the frontal/parietal area, there is often a period of apparent concussion that may last minutes to hours. The most severely affected animals transiently lose all reflexes and are sometimes thought to be dead. Even after recovery of consciousness, such horses are typically obtunded for up to several hours. Altered behavior (i.e., dementia) is another characteristic of forebrain injury: A suckling foal may lose affinity for its dam; the horse may fail to respond to training cues; and the horse may exhibit yawning, head pressing, compulsive walking (often in circles around the inside of an enclosure, usually toward the side of the injury), or, in rare cases, hyperexcitability or aggression. Because of damage to the visual centers in the occipital cortex, vision and the menace response may be impaired in the eye contralateral to the lesion; however, pupillary light reflexes are usually intact. Injury to the somesthetic centers of the parietal cortex interferes with awareness of (and thus response to) touch on the opposite side of the head in a manner analogous to the way in which trauma can cause cortical blindness and an abnormal menace response. This perception of touch is best evaluated by comparing the horse's reactions to tapping the nasal septal mucosa on either side. Seizures, which occurred in 7 of 34 cases of head trauma in one equine series,15 are likely to be generalized, with loss of consciousness and uncontrolled autonomic activity (e.g., salivation, urination, defecation, pupillary dilatation, chewing movements) and abnormal motor function (e.g., muscular rigidity, followed by running and paddling movements of the limbs).
In comatose horses with cerebral injury, the breathing pattern may be irregular, with periods of either Cheyne-Stokes breathing or hyperventilation.Midbrain injury is a relatively uncommon but serious complication of head trauma of any type. It may occur immediately after the injury or be secondary to subtentorial herniation of forebrain components, rostral herniation of the cerebellum, or intraparenchymal bleeding. Because of involvement of the ascending reticular activating system, affected horses are usually obtunded and may be comatose. Weakness of limbs is observed bilaterally or on the side opposite an asymmetric midbrain lesion. In recumbent horses with severe midbrain injury, the neck, back, and limbs may be rigidly extended in a decorticate posture. If the nucleus of cranial nerve III (oculomotor) is involved, the horse exhibits strabismus and a dilated, unresponsive pupil. With severe diffuse injury, bilateral pupillary miosis may occur initially, followed by gradual progression to fixed, dilated pupils. Vision is normal unless there is involvement of other parts of the brain.
Vestibular dysfunction is common in horses after poll trauma or THO. Clinical signs may arise because of injury centrally or, more commonly, because of involvement of the vestibular apparatus or vestibulocochlear nerve (cranial nerve VIII). Peripheral vestibular disease is characterized by head tilt, neck turn, body lean, and staggering in tight incomplete circles, all toward the side of the lesion. These signs can be revealed or exacerbated by blindfolding. With acute severe vestibular dysfunction secondary to THO, recumbency may occur suddenly, with flailing and thrashing movements. These signs of vestibular disease can easily be mistaken for seizures. The ipsilateral eye is usually rotated ventrally and laterally, especially when the horse's nose is elevated, and horizontal or rotatory nystagmus may occur, with the fast phase away from the side of the lesion. Facial paralysis is attributable to damage to cranial nerve VII as it passes close to the middle/ inner ear. With central vestibular disease, signs are similar to those observed when the injury is peripheral; however, additional signs suggestive of brainstem damage may also be present, including spontaneous vertical nystagmus, signs of other cranial nerve dysfunctions, obtundation, and limb ataxia and weakness. In horses, central lesions quite commonly result in a paradoxical vestibular syndrome in which the lesion (usually in the caudal cerebellar peduncle or the flocculonodular lobe of the cerebellum) is located on the side opposite that expected from the clinical signs. An important clue to the presence of this syndrome is the finding of other signs of cranial nerve dysfunction (e.g., facial paralysis) on the side opposite the direction of circling.
In horses with traumatic damage to the pons and medulla of the hindbrain, there is evidence of dysfunction of multiple cranial nerves in association with obtundation and limb ataxia/ weakness. An affected horse may exhibit reduced jaw tone or deviation of the jaw (cranial nerveV [motor]), reduced facial sensation (V [sensory]), facial paralysis (VII), vestibular signs (VIII), dysphagia and respiratory stridor (IX and X), or tongue paralysis (XII). The gait may appear hypometric (spastic), like that in horses with compression of the cervical spinal cord. With severe hindbrain lesions, rapid deep breathing or other abnormal respiratory patterns can be observed.
Signs of cerebellar injury are rare and are usually a result of poll trauma. Coarse head tremors are the most consistent sign; these are especially obvious during attempts to eat or suckle (intention tremor). Horses with cerebellar injury typically have a broad-based swaying stance, and limb movements may be hypermetric or spastic, clumsy, faltering, and jerky. Infrequent signs of cerebellar trauma include absence of the menace response with normal vision and paradoxical vestibular syndrome (see earlier description).
With traumatic optic neuropathy (usually after poll trauma), vision and pupillary light reflexes are impaired or absent and pupils are dilated immediately after the injury. Because the secondary phase of nerve injury continues for many hours after the initial trauma, visual function may progressively deteriorate during at least the first 24 hours after trauma. The signs of facial nerve injury depend on the site of damage. Evidence of complete unilateral facial paralysis includes deviation of the nose toward the normal side, reduced flaring of the ipsilateral nostril during inspiration, and ipsilateral drooping of the lip, eyelid, and ear. Reflexes involving cranial nerve VII, such as the lip, eyelid, and ear reflexes, and the menace response are reduced or absent. Inability to close the eyelid causes minimal corneal problems in a horse with normal mentation unless there is also damage to the secretomotor fibers of the facial nerve along its greater petrosal branch or proximal to the geniculate ganglion, in which case interference with lacrimation causes corneal drying (keratitis sicca). Typically, a deep horizontal corneal ulcer develops within hours of the injury. The tongue protrudes out of the paralyzed side of the mouth, which is often misinterpreted as a problem with lingual function. Buccinator (cheek) paralysis causes a form of dysphagia, evidenced by dropping of and accumulation of feed between the teeth and cheeks (quidding). The peripheral parts of other cranial nerves are infrequently damaged with head trauma. The key to distinguishing central from peripheral causes of neurologic deficits is that the former usually involve multiple cranial nerves and are accompanied by obtundation, ataxia, and weakness, which are not found with peripheral lesions.
■ Pathophysiology Impact to the brain causes immediate damage to intracranial vasculature, neuronal cell bodies, axons, and glia.2,20,21 Neuronal depolarization initiated at the site of impact may spread centrifugally throughout the cortex and cause the transient coma characteristic of severe concussion.
In axons, a dramatic rise in intracellular calcium concentration activates processes that cause interruption of axoplasmic flow and result over hours to days in death of the distal axon. Diffuse axonal injury is thought to account for many of the permanent neurologic sequelae of head trauma. These early events constitute primary brain injury. Subsequent damage occurring during the response phase is termed secondary injury.
The surface and parenchyma of the brain may be lacerated by fracture fragments pushed inward from the calvaria. Significant bleeding at any site compresses the brain against the skull, thereby raising intracranial pressure (ICP). Extravasated blood also elicits inflammatory responses in glial and other cells, initiating many of the auto destructive cascades that characterize the secondary phase of traumatic brain injury. Bleeding, ischemia, and mechanical damage to tissues result in liberation and production of vasoactive and other media- 2022
tors.20,22 The production and action of damaging mediators is much affected by brain temperature: Adverse effects are muted in the presence of hypothermia and are exacerbated by increased temperature.
Hemorrhage, increased permeability of damaged vasculature, and inflammatory edema all increase extravascular volume at the expense of brain volume. Exuberant swelling of the relatively mobile cerebral hemispheres may force portions under the falx cerebri (if asymmetric) or tentorium cerebelli.20,21 In extreme cases, the pressure of subtentorial herniation in turn pushes the caudal cerebellum through the foramen magnum. The effects of reduced systemic blood pressure and increased ICP combine to choke off oxygen and glucose supply to cells and prevent removal of cellular metabolites such as lactic acid.22 The consequent tissue hypoxia is more severe if blood oxygen
content is also reduced, as may occur after traumatic blood loss that results in anemia or hypoxemia.
In the hypoxic environment of the traumatized brain, neuronal adenosine triphosphate (ATP) is depleted rapidly, and energy-dependent homeostatic systems of membranes collapse.22 Calcium and sodium ions flow into cells in response to changes in membrane ion channel function associated with energy depletion, damage by reactive oxygen species, and the actions of glutamate/aspartate. Brain damage that occurs during the primary traumatic event is irreversible; however, there is a window of minutes to days in which equally important secondary injuries theoretically can be prevented or treated.
■ Diagnosis Changes in routine hemograms and chemistry profiles are nonspecific. Collection of CSF from the atlantooc- cipital cistern is generally contraindicated in head trauma because of concern about inducing cerebellar herniation, but CSF can be collected via the lumbosacral space. Characteristic changes include xanthochromia, high RBC count, and high protein levels with normal nucleated cell counts.
Conventional diagnostic radiography is the best and most practical method for initial evaluation of skull trauma; on radiographs, however, the extent of bony and soft tissue abnormality is significantly underrepresented. Because the brain is not visible in plain radiographs, degrees of brain injury must be inferred from secondary changes in the skull. Fractures are visible as radiolucent lines within the calvaria; however, such lines may be characteristic of normal suture lines. A step defect is visible when the fracture fragments are misaligned. Lateral views are most useful for detecting parietal/frontal and basilar fractures and for finding bone fragments originating from the basisphenoid or nuchal crest. On dorsoventral images, a thickened stylohyoid or radiodense osseous bulla is most easily appreciated. Increased opacity of the affected bulla may reflect hemorrhage into the middle ear in association with petrosal bone injury, or it may reflect reactive thickening of the ventral bulla wall in cases of THO. Intracranial or spinal intrathecal gas shadows may be visiable if a communication exists between the subarachnoid space and the skin surface, nasal cavity, paranasal sinuses, or middle ear. Bleeding into the paranasal sinuses, guttural pouches, or retropharyngeal area may be radiographically evident. In cases of frontal/parietal impact, it is also prudent to obtain radiographs of the cervical spine so as to detect fractures/dislocations caused by the axial compressive force of the original impact.
On computed tomography (CT), characteristics of brain trauma include change in ventricular size, shape, or position; deviation of the falx cerebri (falx shift); and focal change in brain opacity.23 Extrdural, subdural, and subarachnoid hemorrhages may each be appreciated as discrete lines between the cortical surface and skull. Administration of iodinated contrast medium intravenously causes focal enhancement of areas of brain injury or hemorrhage. CT is particularly useful for identifying fractures of the bones that surround the caudal fossa; such fractures are often not well depicted by conventional radiography.24 They include fractures of the petrosal bone, basilar and sphenoid bones, occipital condyles, and squamous temporal bone.16 Blood in the middle ears, paranasal sinuses, guttural pouches, or retropharyngeal tissues and changes associated with THO are also easily observed. The principal disadvantage of CT in North America, apart from high cost and limited availability of necessary equipment, is the need for general anesthesia. In Europe, and increasingly in North America, CT of the skull can be performed in standing, unanethsetized animals.
The main advantages of magnetic resonance imaging (MRI) over CT include lack of beam-hardening artifacts, ability to acquire images in any plane, and higher sensitivity for detection of early infarcts and edema. CT is more sensitive than MRI for detection of bony abnormalities, acute brain hemorrhage, and intracranial gas. The brain is not accessible to ultrasound imaging; however, the technique is sometimes useful for assessing fractures of the skull.
Clinical findings and historical information may form the sole bases for diagnosis in many cases.
■ Treatment Relevant treatments for brain injury can be classified in two levels according to evidence-based support for their use. All applicable level 1 treatments should be used in every case of clinically apparent brain injury, whereas level 2 treatments are less clearly indicated and can be considered optional.
LEVEL 1
Treat Other Injuries or Diseases. The normal principles of critical care medicine apply to the brain-injured patient: Establish an airway, obtain vascular access, clean and dress wounds, stanch the bleeding, sedate the horse if necessary, and move the horse to a cool, well-padded area. If necessary, a padded helmet can be used to minimize additional head trauma. A regimen of broad-spectrum antibiotics should be begun if the horse has an open wound or fracture.
Treat Hyperthermia. Hyperthermia after head trauma results from either a resetting of the hypothalamic temperature set point (fever) or excessive heat production in horses with normal set points. High brain temperature accelerates all of the destructive forces unleashed during the secondary phase of brain injury, and so it must be detected and treated vigorously. Rectal temperature should be checked frequently, and efforts at cooling should begin when the rectal temperature exceeds 38° C (101° F). In brief, ambient temperature can be reduced, the hair can be clipped, ice water or isopropyl alcohol can be repeatedly applied to and removed from the skin (including the head), and overhead or box fans can be placed close by. Antipyretic medication (e.g., flunixin meglumine, 1.1 mg/kg IV bid or sid) is particularly useful when the horse has a fever but should be tried in all cases of hyperthermia. NSAIDs have the additional advantages of analgesic and antiinflammatory action.
Prevent or Treat Hypotension. Blood pressure must be normal or close to normal to sustain adequate cerebral perfusion. The old notion that patients with head trauma should be “kept a little dry” is no longer viable. Blood pressure should be monitored frequently, and heart base-adjusted systolic blood pressure should be maintained above 110 mm Hg.25 Blood volume should be maintained or expanded by IV infusion of isotonic (Normosol-R; Plasma-Lyte A; lactated Ringers solution) or hypertonic (hypersaline) crystalloid or colloid (plasma, hetastarch) solutions. Plasma may have additional useful effects, including antioxidant and protease-inhibiting activities. In the case of significant blood loss, cross-matched whole blood is the fluid of choice. If volume resuscitation alone is inadequate to restore normal pressure, pressor/inotropic drugs may be used (e.g., dopamine, dobutamine, norepinephrine).25 The effects of these drugs on cerebral vascular tone, however, are difficult to predict.
Optimize Oxygen Content of Blood. Oxygen is carried in blood either bound to hemoglobin (predominantly) or as free gas. Thus it is important that both hemoglobin concentration and partial pressure of arterial oxygen (PaO2) are at least in the normal range. Hypoxemia (arterial oxygen saturation, however, the efficacy and safety of this approach have not been established. Hemoglobin concentration must be kept above at least 7 g/dL (packed cell volume of 21%) and probably above 11 g/dL. Anemia can be treated with whole blood (preferable in the case of blood loss anemia) or packed RBCs.
Ensure Adequate Pulmonary Ventilation. High Pco2 has the potential to exacerbate CNS acidosis and cerebral edema. In foals, hypercapnia can be addressed by mechanical ventilation of the lungs. In all horses with head trauma, pulmonary ventilation must be optimized by ensuring a patent airway and treating lung disease. For example, acute pulmonary edema may be treated with furosemide (0.5 to 1 mg/kg IV q8h or continuous rate infusion). Ventilation-induced hypocapnia has been advocated as a way to lower ICP26; however, low Pco2 may cause reflex cerebral vasoconstriction and probably should not be used in foals with brain injury.
Control Pain. Alleviating pain in brain-injured horses not only is humane but also may reduce ICP.27 An NSAID (e.g., flunixin meglumine, 1.1 mg/kg IV or PO bid) or opioid (e.g., morphine, 0.1 to 0.3 mg/kg IV or IM qid) can be used for this purpose. Useful analgesic effects have also been achieved with constant-rate infusion of butorphanol or lidocaine.
Regulate Blood Glucose and Maintain Nutrition. Experimental studies have shown that at least 140% of maintenance energy is expended by animals with severe brain injury.28 Even during the first 24 hours after injury, nutrition (enteral or parenteral) probably should be provided to anorexic horses with head trauma. Blood glucose concentration ought to be kept greater than 80 mg/dL in order to provide adequate substrate for brain cells and less than 180 mg/dL so as to prevent hyperglycemia-induced exacerbation of CNS acidosis and apoptosis of brain cells. Dextrose and regular insulin can be infused IV as needed to maintain normal blood glucose concentration.
Prevent or Treat Brain Swelling. If possible, the neck should be free of constrictive wraps and only one jugular vein should be punctured or catheterized in order to prevent obstruction of venous flow from the head. Likewise, any recumbent horse should have its head elevated at least 10 degrees in order to facilitate blood flow. If the horse is significantly depressed (i.e., at least stuporous) or has signs of worsening brain function, a hyperosmolar infusion should be given to try to reduce the extravascular volume of the brain. The solution of choice is hypertonic saline (e.g., 1232 mmol Na/L), which is given as a continuous IV infusion of 1 mL (1.2 mmol)/kg/h for 6 hours and then 0.2 mL/kg for another 12 hours. Alternatively, boluses of 2 mL/kg can be given q4h in five infusions. Further treatment with hypertonic saline should be based on reassessment of clinical signs and plasma sodium concentration (keep sources of thiaminases are bracken fern (Pteridium aquilinum), horsetails (Equisetum arvense), and toxic doses of amprolium (e.g., 400 to 800 mg/kg/day). The clinical signs of thiamine deficiency are ataxia, conscious proprioceptive deficits, heart block, bradycardia, blindness, weight loss, dysuria, hypothermia of the extremities, and periodic muscular fasciculations. In affected horses, convulsions are a terminal development. Electrolyte changes include hyperkalemia, hyperphosphatemia, hyperglycemia, and decreased glucose tolerance. Parenteral thiamine is an effective treatment.1,2
More on the topic Trauma to the Brain and Cranial Nerves:
- Smith Bradford P., Van Metre David C., Pusterla Nicola (eds.). Large Animal Internal Medicine. Part 2. 6th edition. — Elsevier,2020. — 2279 p., 2020
- Blindness and Ocular Abnormalities
- Abnormalities of Cranial Nerve Function
- Upper Motor Neuron Disease
- ENTERAL NUTRITIONAL SUPPORT
- Organization of the Nervous System
- Eyeball position and movement
- Neuroanatomy and lesion localisation
- Diseases Manifesting Principally With Forebrain Dysfunction or Multiple-Level Brain Dysfunction
- Neural Control of Skeletal Muscle