Laboratory tests for the diagnosis of exocrine pancreatic disorders
Jorg M. Steiner
1.4.4.1 Introduction
Exocrine pancreatic disease is common in both dogs and cats. In a study of necropsy findings, 1.5% of 9,342 canine pan- creata and 1.3% of 6,504 feline pancreata examined at necropsy showed significant pathological lesions.1 Pancreatitis is the most common exocrine pancreatic disorder in both species, followed by exocrine pancreatic insufficiency, exocrine pancreatic neoplasia, and rare conditions of the exocrine pancreas.
Pancreatitis is also common in human beings. A recent study reported that 300,000 patients are discharged from the hospital each year with a diagnosis of pancreatitis in the USA alone.2 This number does not include patients that only have mild forms of pancreatitis and are not admitted to a hospital or those that have severe disease leading to death. In addition, it has been estimated that approximately 90% of all cases of pancreatitis in human beings remain undiagnosed. It is likely that the number of undiagnosed cases in dogs and cats is at least as high as in human beings. Reasons for the difficulty of diagnosing exocrine pancreatic disease are the nonspecific clinical picture, the lack of specific changes on routine blood work, the low yield of diagnostic imaging in making a definitive diagnosis, and until recently, the lack of sensitive and specific markers for pancreatic function and pathology.1.4.4.2 Pancreatitis
Serum amylase and lipase activities
Serum amylase and lipase activities have been used for several decades to diagnose pancreatitis in both human beings and dogs. Unfortunately, neither one of these diagnostic tests is both sensitive and specific for pancreatitis. After total pancreatectomy in dogs significant serum amylase and lipase activities remain, clearly indicating that there are other sources of serum amylase and lipase activity than the exocrine pan- creas.3 This lack of specificity is also reflected by clinical studies that showed a specificity of serum amylase and lipase activities for pancreatitis of only approximately 50%.4 Many non-pancreatic diseases, such as renal, hepatic, intestinal, and neoplastic disease can lead to increases in serum amylase and lipase activities.5 Steroid administration can also lead to an increase in serum lipase activity and a variable response in serum amylase activity.6,7 Thus, in dogs, serum amylase and lipase activities are only of limited clinical usefulness for the diagnosis of pancreatitis and should only be used until a more definitive diagnostic test, such as abdominal ultrasound, serum canine pancreatic lipase immunoreactivity (cPLI) concentration, or even exploratory laparotomy can be performed.
Serum amylase and/or lipase activities that are 3-5 times the upper limit of the reference range in patients with clinical signs consistent with pancreatitis, are suggestive of pancreatitis. However, it is important to note that approximately 50% of dogs with an elevated serum lipase and /or amylase activity do not have pancreatitis. In cats, serum amylase and lipase activities appear to be of no clinical value for the diagnosis of pancreatitis.8 While cats with experimental pancreatitis showed an increase in serum lipase activity and a decrease in serum amylase activity, these changes were not seen in cats with spontaneous disease.8,9Serum trypsin-like immunoreactivity (TLI)
TLI concentration is a specific marker for exocrine pancreatic function. Serum TLI mainly measures trypsinogen, the only form of trypsin that circulates in the vascular space in healthy individuals. In addition, if present in serum, the TLI assay also measures trypsin and a portion of trypsin bound to some proteinase inhibitors. In healthy animals, serum TLI concentration is low as most of the trypsinogen synthesized by pancreatic acinar cells is released into the pancreatic duct and does not reach the vascular space (Figure 1.45). During pancreatitis an increased amount of trypsinogen leaks into the vascular space, which leads to an increase in serum TLI concentration.10 Trypsin, which is prematurely activated during pancreatitis, may also contribute to this increase in serum TLI concentration. However, both trypsinogen and trypsin are small molecules that are quickly cleared by the kidney. In addition, any prematurely activated trypsin is quickly removed by proteinase inhibitors, such as α1-proteinase inhibitor (α1-PI) and α2-ma- croglobulin. In turn, α2-macroglobulin-trypsin complexes are removed by the reticuloendothelial system, mainly in the spleen and the liver. Therefore, the serum half life for TLI is short and a significant degree of active inflammation is required in order to have an increased serum TLI concentration.
Also, some patients with peracute severe disease may have normal serum TLI concentrations. One possible explanation for this phenomenon is that not enough trypsinogen remains in the acinar cells to leak into the vascular space. In dogs, serum canine TLI (cTLI) concentration is of limited clinical usefulness for the diagnosis of pancreatitis. While it is more specific than serum amylase and lipase activity, its sensitivity is lower and for most veterinarians the turnaround time for this test is longer than that for serum lipase and amylase activities, thus making the measurement of serum cTLI less desirable as a diagnostic test for pancreatitis.4 The sensitivity and specificity of serum TLI concentration in dogs and cats is similar with a specificity of approximately 90% and a sensitivity of 30-40%. While these performance indices are less than ideal, until recently, serum feline TLI (fTLI) concentration was the most sensitive and specific diagnostic test for feline pancreatitis avai- lable.10 Abdominal ultrasound is also highly specific for pancreatitis if stringent criteria are applied, but the sensitivity of abdominal ultrasound is only between 10% and 35% in cats, and was lower than the sensitivity for serum fTLI concentration in every study in which both diagnostic parameters were evaluated.10,11
Pancreatic lipase immunoreactivity (PLI)
Serum PLI specifically measures the mass concentration of classical pancreatic lipase in serum, rather than its kinetic activity. Assays for the measurement of PLI in dog and cat serum have recently been developed and validated.12,13 Serum PLI concentration has been shown to be highly specific for exocrine pancreatic function in both species.14 Serum cPLI concentration has also been shown to be far more sensitive for the diagnosis of pancreatitis than any other diagnostic tool available.15 Sensitivity for serum PLI concentration has been reported at 82% in the dog and at 67% to 100% in the cat.15,16 Currently, measurement of serum fPLI concentration is only available through the Gastrointestinal Laboratory at Texas A&M University.
However, a commercial assay for the measurement of cPLI concentration (Spec cPL®; Idexx Laboratories) has recently been introduced and performs the same as the original cPLI ELISA. Also, in-clinic assay kits for measurement of cPLI and fPLI, respectively, should be available in the near future. The current control range for serum cPLI concentration as measured by the Spec cPL assay is ≥200 μg∕L, with a diagnostic cut-off value for canine pancreatitis of 400 μg∕L. The current control range for fPLI concentration as measured by radioimmunoassay (RIA) is 1.2 to 6.8 μg∕L with a diagnostic cut-off value for feline pancreatitis of 12 μg∕L. Serum PLI concentrations between 200 and 399 μg∕L in dogs and 6.9 to11.9 μg∕L in cats are considered in the questionable range, requiring repeat analysis and ∕or further diagnostic tests. Chronic renal failure has been shown to have no clinically significant effect on serum cPLI concentration.17 Therefore, the assay can be used to diagnose pancreatitis in dogs with renal failure, underscoring the high specificity of this new diagnostic test. While this has not been confirmed in cats, there is little reason to believe that this would be different in this species. Also, oral administration of long-term high-dose prednisone (2.2 mg∕kg daily for 4 weeks) did not alter serum cPLI concentration.
Other tests for the diagnosis of pancreatitis in dogs and cats have been evaluated. However, plasma trypsinogen activation peptide (TAP) concentration, urine TAP concentration, urine TAP∕creatinine ratio, serum α1-PI∕trypsin complex concentration, and serum α2-macroglobulin concentration have all been shown to be of little clinical usefulness for the diagnosis of spontaneous pancreatitis in dogs or cats.4
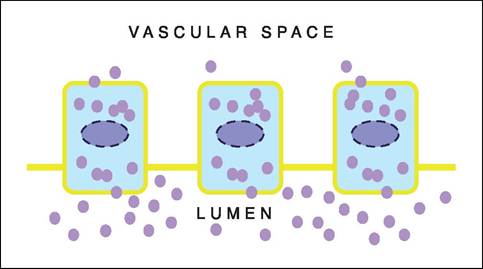
Figure 1.45:
Physiology of pancreatic enzyme secretion.
Acinar cells secrete zymogens (e.g., trypsinogen) and pancreatic enzymes (e. g., pancreatic lipase) into the duct system of the exocrine pancreas, ultimately reaching the duodenum. However, a small amount of zymogens and enzymes is also secreted into the vascular space and can be measured by species-specific immunoassays.1.4.4.3 Exocrine pancreatic insufficiency (EPI)
In the past, several fecal tests have been used to diagnose EPI. Microscopic fecal examination for fat and∕or undigested starch or muscle fibers may suggest maldigestion, at best. In light of the wide-spread availability of tests with high accuracy for the diagnosis of EPI, microscopic fecal examination can no longer be clinically justified. Fecal proteolytic activity had been used for several decades to diagnose EPI in small animals. Several variations of the test have been described, the most simple involving digestion of the gelatin emulsion on a piece of radiographic film. Most of these methodologies, particularly the radiographic film clearance test, are completely unre- liable.18 One method, which utilizes pre-made tablets that can be used to pour a gelatin agar, has been found to be most useful.18 However, false positive as well as false negative results have been reported and the clinical use of fecal proteolytic activity should be limited to species for which more specific assays to estimate pancreatic function are not available.
Serum trypsin-like immunoreactivity (TLI)
Serum TLI is the diagnostic test of choice for EPI in both dogs and cats.19,20 Assays for TLI measure trypsinogen, the zymogen of trypsin, circulating in the vascular space. In healthy individuals only a small amount of trypsinogen is present in serum (Figure 1.45). In dogs and cats with EPI, serum TLI concentration decreases significantly and may even be undetectable (Figure 1.46). The reference range for serum canine TLI (cTLI) concentration is 5-35 μg∕L with a cut-off value for EPI of ≤2.5 μg∕L.
Similarly, the reference range for serum66 Diagnostic Tools
id="Picutre 51" class="lazyload" data-src="/files/uch_group31/uch_pgroup24/uch_uch7224/image/image051.jpg">
Figure 1.46:
Serum TLI in dogs and cats with EPI. Dogs and cats with EPI have a severely decreased functional mass of the exocrine pancreas. As a result, the secretion of digestive enzymes may be decreased to a point that maldigestion ensues and clinical signs of EPI become apparent. At the same time, leakage of trypsinogen into the vascular space is reduced and serum TLI concentration is decreased below the cut-off value for EPI.
not be diagnosed, the serum TLI concentration should be reevaluated after a couple of months in these patients.
Serum pancreatic lipase immunoreactivity (PLI)
Similarly to serum TLI concentration, serum PLI concentration is highly specific for exocrine pancreatic function and could be used for the diagnosis of EPI.14 However, there is a small degree of overlap for serum cPLI between normal dogs and dogs with EPI, making the measurement for PLI slightly inferior to TLI for a definitive diagnosis of EPI. The only exception to this is the rare patient with an isolated pancreatic lipase deficiency. Since pancreatic lipase is essential for fat digestion, clinical signs of maldigestion may ensue in these rare cases. The clinical utility of serum fPLI concentration for diagnosis of feline EPI has not been evaluated to date.
Fecal elastase
feline TLI (fTLI) concentration is 12-82 μg∕L with a cut-off value for EPI of ≤8.0 μg∕L. Rarely, animals with a serum TLI concentration below the cut-off value are encountered that do not have clinical signs of EPI. This is probably due to the large functional reserve of the gastrointestinal tract. On the other hand, there are many dogs and cats with chronic diarrhea and weight loss that have a mild decrease in serum TLI concentration (2.6 to 4.9 μg∕L in dogs, 8.1 to 11.9 μg∕L in cats). Most of these animals have chronic small intestinal disease and should be worked-up accordingly. A small number of these dogs and cats may have EPI and if small intestinal disease can-
Recently, an assay for measurement of fecal elastase has been developed and validated. Fecal elastase concentration has a lower specificity than measurement of serum cTLI concentra- tion.21 Since the prevalence of EPI in dogs with chronic diarrhea and weight loss is only approximately 10%, the number of false positive test results for fecal elastase concentration is unacceptably high (23.1% in a recent study). Also, measurement of fecal elastase concentration is more cumbersome and more expensive than the measurement of serum cTLI concentration. The only scenario in which fecal elastase concentration may be clinically useful is a patient with EPI due to obstruction of the pancreatic duct. However, this condition has not been described in dogs or cats to date.
of clinical disease, allow for selective breeding, and can also identify susceptible animals so that onset of disease can be delayed or prevented by prophylactic intervention.
Selective breeding for appearance has reduced the genetic diversity within breeds of pedigree dogs, and in some breeds it has unintentionally increased the likelihood of inheriting gene mutations that cause disease or disease susceptibility. Over 400 inherited disorders have already been identified in dogs, and it seems certain that many more will be characterized.1,2 Sequencing and mapping the entire canine genome is well advanced, providing the tools to identify genomic markers for inherited diseases in dogs.3,4 The situation in the cat is different as the majority of cats are domestic shorthair cats. As a consequence, there has been little selective breeding and there are few known inherited disorders in cats.5
There is considerable potential for the application of molecular-genetics-based tests for gastrointestinal disorders in dogs, underlined by emerging knowledge of inheritance and pathogenesis of the many breed-associated conditions already described (Table 1.11). Currently, the mode of inheritance has been identified in a few, and the genetic abnormality in only one instance.6 The barriers to progress include the complex nature of many gastrointestinal disorders, for some of which there may be environmental factors operating with genetic drivers of disease.
1.4.5.2 Test Development
Molecular-genetics-based tests are typically dependent on the identification of DNA markers or mutations within or close to key genes that drive specific traits or diseases. These tests are performed on genomic DNA extracted from cheek swabs or whole blood. Identification of mutations in the gene or genes involved could be considered to provide the ultimate reliable test. This can be achieved by a candidate gene approach, based on genes that have been identified in similar conditions in other species or by knowledge of the pathophysiology of the disease. Alternatively, DNA markers within or in close proximity may be used to detect abnormal genes. Informative microsatellite markers may be identified by linkage analysis, which relates a specific allele of a particular microsatellite marker with disease. This approach is used when candidate genes are either unknown or uncertain. Alternatively, informative SNPs (single nucleotide polymorphisms) can be identified by association studies.
There are many practical considerations in the development of molecular-genetics-based tests for gastrointestinal diseases in dogs. The most important is accurate characterization and identification of the target phenotype that should be distinct (for example, EPI or hepatic copper toxicosis). A distinct phenotype facilitates accumulation of data from extended families to determine inheritance and for linkage analysis. Clearly, development of genetic tests is much more difficult for conditions that are less distinct or that are multifactorial, such as IBD. However, provided there is an inherited component, other types of molecular-genetic studies can be done in large numbers of unrelated dogs; for example, using disequilibrium linkage analysis of microsatellite data, SNPs, or sequencing of candidate gene(s). Results from these studies may in fact help to redefine the phenotype.
Complexity of inheritance is also important. Tests for single gene disorders are easiest to develop and most likely to be used not only to identify but also to eliminate a condition by selective breeding. Complex genetic diseases are at the other end of the spectrum, where multiple genes drive disease susceptibility and disease expression may depend on an environmental component, such as an allergen or pathogen. Selective breeding with the goal of elimination is not a practical option for complex genetic diseases, but genetic tests may direct treatment and preventative strategies.
Table 1.11: Putative and / or proven inherited gastrointestinal diseases of dogs
| Disease | Breeds | Inheritance |
| Intestinal | ||
| ■ Basenji enteropathy | Basenji | Not known |
| ■ Gluten-sensitive enteropathy | Irish Setter | Autosomal recessive |
| ■ Histiocytic ulcerative colitis | Boxer dogs | Not known |
| ■ Idiopathic small intestinal bacterial overgrowth | Beagle German Shepherd | Not known |
| ■ Lymphangiectasia | Norwegian Lundehund | Not known |
| ■ Protein-losing enteropathy | Soft-coated Wheaten Terrier | Not known |
| ■ Selective cobalamin malabsorption | Beagle Border Collie Giant Schnauzer Shar Pei | Autosomal recessive |
| Pancreatic | ||
| ■ Exocrine pancreatic insufficiency | German Shepherd | Autosomal recessive |
| Hepatic | ||
| ■ Copper | Bedlington Terrier | Autosomal recessive |
| hepatotoxicosis | ||
| Dalmatian | Not known | |
| Labrador Retriever | Not known | |
| Skye Terrier | Not Known | |
| West HighlandWhiteTerrier | Not Known | |
| ■ Portovascularanomalies: | ||
| - Intrahepatic shunt | Irish Wolfhound | Autosomal recessive |
| (single gene) | ||
| - Extrahepatic shunt | Cairn Terrier | Autosomal recessive |
| YorkshireTerrier | Not known | |
| ■ Microvascular | Terrier breeds | Not known |
| dysplasia | ||
1.4.5.3 Diseases of the esophagus and stomach
Little is known about the genetics of these diseases in dogs. Breed predispositions for gastric dilation/volvulus are most likely related to anatomical features (large, deep-chested dogs). Antral gastric hypertrophy has been described as a congenital disorder in small brachycephalic dogs, but there is not enough information to describe this condition as an inherited trait.
1.4.5.4 Intestinal diseases
Selective cobalamin malabsorption
Selective intestinal malabsorption of cobalamin (vitamin B12) accompanied by proteinuria is inherited as a simple autosomal recessive trait in Giant Schnauzers, and has also been described in Beagles, Border Collies, and Shar Peis.7,8,9 Affected puppies show chronic inappetence and failure to thrive, and have low serum cobalamin concentrations, megaloblastic anemia, and methylmalonic aciduria. Clinical signs can be reversed with parenteral, but not oral, cobalamin supplementation. These patients have a defective expression of the intrinsic factor-coba- lamin receptor (IFCR) in the ileal brush border membrane, which has been attributed to mutations affecting either of the two proteins (cubilin, amnionless) that mediate endocytosis of the IF-cobalamin complex.10
Gluten-sensitive enteropathy (GSE)
GSE is a well-characterized small intestinal disease in Irish Setters, and potentially other breeds of dogs, which can cause weight loss with or without diarrhea.11,12 GSE has several similarities with human celiac disease, which involves immune- mediated damage of the small intestine, but differs because it does not correlate with MHC II haplotypes.11 GSE in Irish Setters has been shown to be inherited at a single autosomal recessive locus, but currently there is no DNA test available.12
Lymphangiectasia
This disease has an increased prevalence in Yorkshire Terriers, Soft-coated Wheaten Terriers, and Norwegian Lundehunds, but can also occur in many other breeds. Familial occurrence has been demonstrated in the Norwegian Lundehund,13 but the mode of inheritance is unknown.
Protein-losing enteropathy (PLE)
PLE can occur in many breeds and in many disease processes, but a distinctive familial predisposition for both PLE and /or PLN has been recognized in Soft-coated Wheaten Terriers.14 Pedigree analysis suggests a common male ancestor, but the mode of inheritance is as yet unknown.
Basenji enteropathy
Basenji enteropathy is a severe form of IBD in Basenji dogs, which closely resembles the non-secretory form of human immunoproliferative small intestinal disease.15 Asymptomatic Basenji dogs can have abnormal intestinal function and gastrointestinal lesions on biopsy. This disease is likely to have a hereditary basis, although the mode of inheritance is unclear.
Small intestinal bacterial overgrowth (SIBO)
SIBO is characterized by relatively high numbers of bacteria in the lumen of the upper small intestine. It is frequently associated with a change from an aerobic to a predominantly anaerobic flora.16 SIBO has recently been named “antibiotic- responsive diarrhea” by some authors.17 SIBO may occur as an idiopathic abnormality, secondary to other gastrointestinal diseases, or as a subclinical finding in apparently healthy Beagle and German Shepherd dogs.16 While German Shepherds appear to have a predisposition to SIBO, its inheritance has not been established. Development of molecular marker(s) for predisposition may be facilitated by identification of a key driver of disease, such as defective intestinal protection due to deficiency or dysregulation of secretory IgA.18
Histiocytic ulcerative colitis
This disease is a form of inflammatory large bowel disease that occurs predominantly in Boxer dogs, although it also has been reported in a few Bulldogs and other breeds. Inheritance has not been established, but a genetic predisposition is suggested by its strong breed predisposition. Pathologically, it is characterized by colonic mucosal ulceration and a mixed inflammatory infiltrate typically including PAS-positive macrophages. The immunohistochemical changes are similar to those reported in human ulcerative colitis. Recent studies suggest that an infectious agent responsive to antibiotics plays an integral role in the clinical manifestation of this disease.19
Inflammatory bowel disease (IBD)
There are many potential causes of this disease phenotype, which is likely to involve a complex interaction of genetic predisposition and environmental factors, such as intestinal microflora and dietary antigens. The genetic background in dogs is obscure but there is emerging evidence of susceptibility due to gene mutations in human beings.20
1.4.5.5 Pancreatic disease
Pancreatic acinar atrophy (PAA)
PAA is the most common cause of EPI in the dog, and is mainly seen in German Shepherd dogs and Rough-coated Collies. Recent studies suggest that PAA may occur as the end stage of lymphocytic pancreatitis.21 PAA has been shown to be a hereditary disease in German Shepherd dogs, most likely due to an autosomal recessive gene.22
Pancreatitis
Hereditary pancreatitis has been described in human beings and several mutations have been associated with an increased risk for pancreatitis. Chronic pancreatitis is also commonly seen in the Miniature Schnauzer, which may be due to the increased incidence of fasting lipidemia and hypertriglyceridemia in this breed. However, screening for mutations of the anionic and cationic trypsinogen genes has not revealed any associations.
ted to be due to a deletion in the MURR1 gene, paving the way for the development of an accurate DNA test.6 The microsatellite C04107 lying in an intron of the MURR1 gene is highly associated with the disease but shows haplotype diver- sity.24 The only solid molecular test for the disease is thought to be by showing the deletion in exon-2 in cDNA in liver tissue; this test is not robust on RNA from peripheral leukocytes because of their low MURR1 expression level. A quantitative PCR (Q-PCR) test on genomic DNA was shown to correlate well with the microsatellite marker and with RT- PCR data from blood samples, buccal swabs, and liver biop25
sies.
A familial copper-associated liver disease that has recently been described in Dalmatians also may involve a primary metabolic defect in copper metabolism, but the mechanism and genetic basis for the disease have not been assessed. There is, furthermore, evidence for different forms of familial copper- associated liver disease in West Highland White and Skye Terriers, but in these dogs inflammatory changes precede copper accumulation, suggesting a different pathogenesis than in Bed- lington Terriers and Dalmatians.
1.4.5.6 Liver disease
Hepatic copper toxicosis
Hepatic copper toxicosis can result either from a primary defect in hepatic copper metabolism or from an altered biliary excretion of copper. An inherited copper storage hepatopathy has been documented in Bedlington Terriers, and there is evidence for familial copper storage liver disease in West Highland White Terriers, Skye Terriers, Dalmatians, Labrador Retrievers, and possibly Doberman Pinschers. Secondary copper accumulation, due to long-standing cholestatic liver disease (copper-associated hepatopathy), may occur in many dog breeds but does not lead to levels high enough to be hepato- toxic. Copper accumulation has been reported in a large number of breeds with cholestatic liver disease in which it is a secondary event. Copper hepatotoxicosis in the Bedlington Terrier is the best-described example of a primary abnormality in hepatic copper metabolism. Accumulation of toxic levels of copper in the liver results in hepatocellular necrosis, hepatitis, and ultimately cirrhosis. This disease has been shown to be autosomal recessive, and has a high prevalence in the breed. Diagnosis used to be by histological assessment and measurement of copper content in liver biopsies. More recently, a microsatellite marker, CO4107, closely linked with the copper toxicosis gene has been used to screen Bedlington Terriers, but this test has been controversial.23 Recently, the copper toxicosis locus has been mapped to canine chromosome 10 at locus CFA 10q28, and the disease has been sugges-
Portovascular anomalies
Congenital portosystemic shunts are characterized by a single anomalous connection between the portal vein and the systemic circulation, bypassing the hepatic sinusoids. Single intra- hepatic shunts are found primarily in large breed dogs, and they are thought to be inherited as a single gene autosomal recessive trait.26 Irish Wolfhounds also may have inherited transient hyperammonemia due to a defect in the urea cycle enzyme arginine succinate synthetase, which should not be mistaken for portovascular anomalies.27,28 Single extrahepatic shunts occur primarily in small dog breeds, especially those having a Terrier heritage. In Cairn Terriers, test matings have shown extrahepatic shunts to be inherited as an autosomal recessive trait, which is most likely polygenic or monogenic with variable expression.29 Portosystemic shunts are also thought to be inherited in Yorkshire Terriers.30
Hepatic microvascular dysplasia (MVD)
MVD is a congenital and probably inherited disorder of the microscopic architecture of the liver, which occurs mostly in small breed dogs, especially Terrier breeds (e.g., Yorkshire, Cairn, and Maltese Terriers). The genetic relationship between MVD and portovascular anomalies is uncertain but considered possible because of their association in certain breeds, similar histological features, and evidence that they may occur together.
??9 Key Facts
■ A breed predilection is commonly observed for gastrointestinal disorders in dogs, but less commonly in cats, suggesting a hereditary nature or effect in the pathogenesis of these diseases.
■ To date the only molecular-based diagnostic test available for the diagnosis of inherited gastrointestinal disorders in dogs or cats is for copper hepatotoxicosis in the Bedlington Terrier.
■ Major advances are to be expected in this field and new diagnostic tests for hereditary gastrointestinal diseases should be available in the near future.
More on the topic Laboratory tests for the diagnosis of exocrine pancreatic disorders:
- Laboratory tests for the diagnosis of exocrine pancreatic disorders
- Contents
- Steiner J.M. (ed.). Small Animal Gastroenterology. Schluetersche,2008. — 387 p., 2008
- Laboratory assessment of gastric disease
- Index
- Preface
- PANCREATITIS
- Alterations in the small intestinal microflora (Small intestinal bacterial overgrowth)
- References
- GRASS INGESTION/ COPROPHAGY/PICA