NEOPLASIA OF THE SMALL INTESTINE
Neoplasia of the small intestine is discussed in detail in Chapter 11. A summary is provided here.
Tumors of the small intestine occur uncommonly. GI neoplasms account for approximately 2% of all canine and feline neoplasms.
Intestinal neoplasms of dogs and cats are usually malignant. Although neoplasia is uncommon overall, in cats intestinal lymphoma is now diagnosed with increased frequency. This is important to recognize because cats with intestinal lymphoma, especially the type now referred to as chronic low-grade lymphocytic lymphoma, often respond well to chemotherapy if the diagnosis is made relatively early in the disease course. The most common malignant neoplasms of the intestinal tract are lymphoma and adenocarcinoma. Other tumors affecting the intestinal tract include mast cell tumor, fibrosarcoma, leiomyoma, leiomyosarcoma, undifferentiated sarcoma, carcinoids, plasmacytoma, and neurolemmoma.Most dogs with intestinal neoplasia are middleage or older (7 years or more). A majority of dogs with lymphoma and adenocarcinoma are males. There is no apparent sex predilection in cats with intestinal neoplasia. Siamese cats appear to be at greater risk for developing adenocarcinoma of the intestine.
The most common clinical signs of intestinal neoplasia are weight loss, vomiting, diarrhea, and lethargy. Inappetence is often apparent as the disease advances. Other signs may include melena, hematemesis, anemia, fever, icterus, and abdominal effusion. Although clinical signs in most patients are slowly progressive, dogs with intestinal adenocarcinoma are occasionally presented because of acute signs that may mimic intestinal obstruction (e.g., acute frequent vomiting, anorexia, lethargy).
Physical examination may reveal pallor, cachexia, thickened intestinal loops, an isolated intestinal mass, intraabdominal lymphadenopathy, dilated intestinal loops, organomegaly (liver, spleen), abdominal effusion, and peripheral edema (most often due to hypoproteinemia associated with diffuse intestinal lymphoma).
Hematologic and biochemical parameters are often normal, although anemia (anemia of chronic disease or anemia consistent with blood loss) and hypoproteinemia may be present. Hypoproteinemia may be due to either blood loss into the intestine or diffuse infiltrative intestinal disease. Neutrophilic leukocytosis and elevated hepatic enzymes may also be present.
Useful procedures in evaluating patients for evidence of intestinal neoplasia include survey radiography, ultrasonography, and endoscopy. Pulmonary metastases are rarely detected on thoracic radiography in patients with small intestinal neoplasia. Survey abdominal radiographs may reveal a soft tissue opacity consistent with a mass or lymphadenopathy, or signs of intestinal obstruction. Contrast radiography can be helpful for delineating regions of significant mucosal irregularity, luminal narrowing, and intramural thickening. Narrowing of the lumen is commonly seen with carcinoma, which has a tendency to be annular (Figure 7-3). Annular indicates that there is 360-degree constriction. Intramural disease usually produces radiographic signs of thickening, rigidity of the wall, and narrowing of the lumen.
Abdominal ultrasonography is useful for defining abdominal mass lesions (e.g., confirming presence of a mass effect, delineating intestinal versus lymph node involvement, examining for hepatic involvement).
A definitive diagnosis of intestinal neoplasia can be made only on histologic examination of biopsy material. Biopsy specimens are most commonly obtained via either endoscopy or exploratory laparotomy. Percutaneous fine-needle aspiration under either ultrasound or laparoscopic guidance can be used in selected cases in which the involved area can be isolated and stabilized for needle insertion. Endoscopy is particularly useful for examining and procuring biopsy samples from the duodenum and terminal ileum. Intestinal lymphoma (either diffuse or focal) can be reliably diagnosed in a majority (approximately 90%) of dogs and cats when proper biopsy instrumentation and technique are used.
Mass lesions can be very reliably diagnosed (samples should be obtained as deeply as possible). Laparotomy offers the advantage of thorough exploration of the abdomen with biopsy and possibly complete excision of involved areas.Intestinal lymphoma in cats and dogs will be discussed here, and the reader is referred to Chapter 11 for a more detailed discussion of neoplasia of the small intestine. Intestinal lymphoma is discussed here as well because clinically it can appear very similar to IBD in cats.
Lymphoma
In cats chronic low-grade lymphocytic lymphoma can be very similar to IBD in the way it manifests itself clinically. It can only be differentiated based on biopsy specimen analysis. Because cats with chronic low-grade lymphocytic lymphoma often have a reasonably good prognosis when indicated treatment is administered, it is incumbent on veterinarians to make the correct diagnosis early in the disease course, rather than later, when it may be more difficult to successfully manage the patient.
The GI tract is a common site of extranodal lymphoma in dogs and cats. In cats intestinal lymphoma is caused by feline leukemia virus, although as few as 12% to 30% have been reported to be viremic. However, more recent studies using PCR methods suggest that the incidence of feline leukemia virus in lymphoma may be as high as 63%. The cause in dogs is unknown. GI lymphoma reportedly arises from B lymphocytes of the gut-associated lymphoid tissue (GALT) in most cases in dogs and cats.

Figure 7-3 Adenocarcinoma involving the ileum of a cat. Note annular constriction and dilation of the segment proximal to the tumor site. (Courtesy Dr. David C.Twedt, Colorado State University, Ft. Collins, Colo.)
Morphologically there are two forms of GI lymphoma: diffuse (multifocal) lymphoma and nodular (solitary) lymphoma. In diffuse lymphoma there is a diffuse proliferation of the lamina propria and submucosa with neoplastic lymphocytes.
The mesenteric lymph nodes are usually affected. There is occasionally deep ulceration of the intestinal mucosa, and malabsorption is common as the disease becomes advanced. The diffuse form occurs commonly in both dogs and cats. In the nodular form a single expanding tumor mass is present that causes progressive luminal obstruction. The most common site is the ileocecocolic region. The mesenteric lymph nodes may or may not be involved.More recently three grades of GI lymphoma have been described in cats. These are referred to as well differentiated (low grade or lymphocytic), poorly differentiated (high grade, lymphoblastic, or immunoblastic), and intermediate (or mixed). Rare forms, such as large granular lymphocytic lymphoma, also exist.
Intestinal lymphoma in dogs and cats is discussed separately because there are both clinico- pathologic and epizootologic differences between the two species. In my experience, cats with intestinal lymphoma respond much better to chemotherapy than do dogs. As a result, I strongly recommend to cat owners that chemotherapy be attempted unless there is significant debilitation at the time of diagnosis. Unfortunately, intestinal lymphoma in dogs is often advanced at the time of diagnosis and malabsorption and panhypoproteinemia are commonly present. Response to chemotherapy is not often very favorable in dogs with advanced disease.
Feline Lymphoma
The most common clinical sign in my series of feline intestinal lymphoma cases is chronic diarrhea. Occasionally, vomiting is the sole or predominant sign (in many of these cats, gastric biopsy results are unremarkable or reveal only mild inflammation), whereas in others vomiting and diarrhea occur with similar frequency. Occasionally the lymphoma involves stomach and/or colon, as well as small intestine. Other signs may include decreased appetite and weight loss (especially as the disease becomes more advanced) and lethargy. Interestingly, some cats have an increased appetite early in the course.
Clinical signs may actually be very similar in cats with hyperthyroidism, IBD, and lymphoma. Therefore it is strongly recommended that middle-age to older cats with chronic (more than 1 to 2 months) GI signs be thoroughly evaluated (complete blood count, biochemical profile, urinalysis, feline leukemia and feline immunodeficiency virus testing, T4 analysis, and endoscopy to obtain GI biopsy samples if hyperthyroidism is not present) to establish a definitive diagnosis.Most cats with intestinal lymphoma are older, with an age range of 6 to 18 years. There does not seem to be a breed or sex predilection. Most cats are domestic short hair cats.
Cats with intestinal lymphoma can survive (and thrive!) for many months to years if the diagnosis is established and chemotherapy is administered early enough. Cats with IBD and lymphoma can demonstrate similar clinical signs. Careful consideration must be given before corticosteroids are used empirically to treat cats with chronic diarrhea.Without question, IBD occurs much more commonly than intestinal lymphoma. Without a histologic diagnosis, however, it is not possible to differentiate a cat with IBD from one with lymphoma. Therefore in middle-age to older cats the best recommendation for owners who wish to do everything possible for their cat is to make a definitive diagnosis before instituting long-term corticosteroid therapy empirically.
Laboratory test results in cats with intestinal lymphoma are variable. Frequently, test results are unremarkable unless there is chronic disease. Abnormalities may include anemia, neutrophilic leukocytosis, lymphocytosis, and hypoproteinemia. Unlike dogs, cats rarely have hypoproteinemia with chronic small intestinal disease. When hypoproteinemia does occur in cats, it is indicative of severe disease, especially when the total protein level is less than 5.5 g/dl. The most common cause of panhypoproteinemia with a total protein of less than 5.0 g/dl in cats is intestinal lymphoma (the primary disorder to rule out is IBD).
Radiographic changes are nonspecific. Abnormalities may include evidence of an abdominal mass or GI obstructive pattern. Contrast studies are not frequently done. Careful abdominal palpation, endoscopy, ultrasonography, and aspiration cytologic analysis of any palpable masses are the most valuable diagnostic aids. Abdominal palpation may be unremarkable or may detect thickened intestines or a mass effect (intestinal mass or lymphadenopathy). Lymphadenopathy is sometimes mild and not readily apparent on palpation. It may occur in conjunction with both IBD and lymphoma. Fine- needle aspiration of a mass may yield sufficient material to make a definitive diagnosis.
Endoscopy is a very safe and reliable means of diagnosing diffuse intestinal lymphoma in cats. Small intestinal masses are not often accessible to endoscopic evaluation, however; if present, exploratory surgery is recommended. As previously stated, aspiration cytologic analysis of a mass may provide a diagnosis, but surgery is still recommended for detailed evaluation and resection of an intestinal mass, where feasible, if there is concern that the mass may cause significant luminal obstruction. Mass resection also provides effective tumor debulking before chemotherapy. Full-thickness intestinal biopsies and mass resection should be done with careful surgical technique, because dehiscence of the suture line may occur. Nonabsorbable suture should be used.
If endoscopy is done, as much of the small intestine as possible is examined. In many cats the tip of the endoscope can be extended to the jejunum. Proper instrumentation and biopsy technique are essential for making a definitive diagnosis of lymphoma on endoscopic biopsy specimen analysis. Gross appearance varies from normal to variable degrees of mucosal irregularity. Erosions or ulcerative changes are occasionally present. As was discussed in the section on IBD, it is sometimes difficult for a pathologist to differentiate diffuse intestinal lymphoma from IBD. This is especially true when severe lymphocytic enteritis is present. Immunoperoxidase studies to assess the clonality of the lymphoid population are often helpful in confirming whether or not lymphoma is present. Pathologists can request that these special stains be done at an academic institution if they are not available at their own laboratory. T-cell and B-cell stains often show presence of virtually 100% of either T lymphocytes or B lymphocytes in lymphoma cases, with a virtually negative stain for the other lymphocyte type. An alternative approach is to proceed to obtaining full-thickness intestinal biopsy samples if it is not clear from evaluation of endoscopic samples what disease process is present.
Lymphocytic-plasmacytic gastroenteritis may constitute a prelymphomatous disorder (see discussion earlier in this chapter in the section on feline IBD). In my experience, however, eventual transition from benign to malignant disease is rare.
There are few detailed reports in the literature of treatment response among cats with GI lymphoma. One recent report described diagnosis and management of 67 cats with GI lymphoma. In this series the histologic grade was determined to be lymphocytic in 75% of cases (50 cats) and lymphoblastic in 25% of cases (17 cats). Several therapeutic protocols have been described. Two of these are discussed here. Multiagent chemotherapy is recommended for all affected cats. Survival times in excess of 12 to 18 months are not unusual. In some cats the response is somewhat shorter (3 to 6 months). The prognosis for longer survival time is much better if the diagnosis is made before clinical signs become chronic and debilitation results. The protocol that I have used most often is described in Table 7-2. This protocol uses cyclophosphamide, vincristine (Oncovin), and prednisolone (COP). It can be easily managed in any practice setting. An alternate protocol that was used in the series of 67 cats used mostly prednisolone and chlorambucil. (See guidelines that follow.)
COP Protocol. Vincristine is administered intravenously at a dose of 0.75 mg/m2 once weekly for 4 consecutive weeks and then once every 3 weeks. The initial doses are often decreased by approximately 25% for cats that are inappetent or debilitated. If well tolerated, the dose can then be
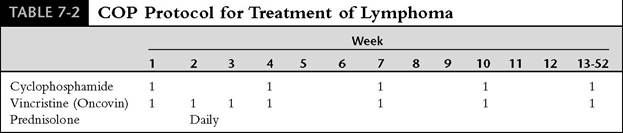
Modified from Cotter SM:Treatment of lymphoma and leukemia with cyclophosphamide, vincristine, and prednisone. II. Treatment of cats, J Am Anim Hosp Assoc 19:159, 1983.
Outline of the COP protocol with current dose recommendations: cyclophosphamide 225 mg/m2 PO (round off to nearest
25 mg on the low side of that dose), vincristine 0.75 mg/m2 IV (see text), prednisolone 1 mg/lb PO continued as long as the cat remains in continuous remission, every 3 weeks for 1 year. For patients 1-5 kg: m2 = 0.5 ? wt in kg + 0.05.
gradually increased. Care is taken to ensure that none of the vincristine is given extravascularly. The average volume that is administered is quite low (0.1 to 0.15 ml for many cats, using a vincristine concentration of 1 mg/ml). Cyclophosphamide is given orally at a single dose of 225 mg/m2 every 3 weeks (50-mg tablets are used, with dose adjusted to the nearest 25 mg on the low side of the calculated dose). Prednisolone is given orally at 1 mg/lb/day. Although cyclophosphamide and vincristine can be given on the same day, I often prefer to have the owner administer the cyclophosphamide 2 to 3 days after the vincristine. This allows a little recovery time between treatments.
A complete blood count is done several times during the first month and then every 3 weeks to be sure that adequate granulocytes are present before treatment. At least 3000 granulocytes∕μl must be present before cyclophosphamide is given. If the granulocyte count drops to less than 1000/ μl 5 to 7 days after cyclophosphamide, the dose for subsequent treatments is reduced by 25%. The highest nontoxic dose is most likely to result in the greatest tumor cell kill.
The COP protocol is generally well tolerated, although side effects may occur and dosage or interval adjustments may be necessary. Side effects of COP in cats may include anorexia, vomiting, lethargy, and severe tissue irritation if any vincristine is given extravascularly. Also, the hair coat may become thinner, but complete hair loss does not occur. Cats do tend to lose whiskers. Cats should be carefully observed for sepsis, especially during the induction phase. Prophylactic antibiotics are not indicated, but any infections that occur should be treated aggressively.
Advantages of this protocol include hospital visits at only 3-week intervals after the first 4 weeks, lower cost to the owner, and a treatment interval that allows recovery of normal cells between treatments. I would like to emphasize that with careful monitoring and use of a dosage schedule that is tailored to each individual cat, few problems are encountered. It is my general practice to encourage owners of most cats with GI lymphoma to pursue treatment that includes chemotherapy.
Nutritional and metabolic support is also important. If inappetence is a problem, cyproheptadine can be administered as an appetite stimulant (1 to 2 mg orally every 12 to 24 hours) on an as needed basis (long-term if necessary). If there is concurrent renal disease with azotemia or if dehydration is a problem, owners are taught how to administer subcutaneous fluids at home (e.g., lactated Ringer's solution, 100 to 150 ml every 24 hours to 48 hours, based on the individual cat's needs). Injections of B-complex vitamins are sometimes helpful as well.
Rarely, chemotherapy can be discontinued after 1 year. This is done only if follow-up endoscopic intestinal biopsy samples indicate that there is no remaining lymphoma. Most cats remain on treatment for the rest of their lives. If chemotherapy is poorly tolerated and reduced dosages and increased intervals between treatment times are unsuccessful in adequately decreasing side effects, chemotherapy should be suspended. Prednisolone should be continued, however, because it may help maintain remission for a period of time. L-Asparaginase can also be used if cyclophosphamide and vincristine are poorly tolerated. Doxorubicin (Adriamycin) can also be used in cats.
Prednisone and Chlorambucil for Lymphocytic Lymphoma. Lymphocytic lymphoma may also be treated with prednisone (or prednisolone) at 10 mg/day orally and chlorambucil (Leukeran) at a dosage of 15 mg/m2 orally once per day for 4 days, repeated every 3 weeks.
Many cats go into remission for a number of months. Cyclophosphamide can be used for “rescue” (225 mg/m2 every 21 days). Adverse reactions on this protocol are rare but may include vomiting, diarrhea, anorexia, and leukopenia.
Monitoring includes running a complete blood count on days 10 and 21 of the first 3-week cycle. If there is no neutropenia (less than 3,000∕μl), the same dosage of chlorambucil is continued. Subsequently a complete blood count is obtained on the tenth day on every second or third cycle thereafter.
Canine Lymphoma
GI lymphomas occur less commonly in dogs than in cats. The GI tract may be involved as either a primary or a secondary site. GI lymphoma appears to be somewhat more common in males than in females.
Clinical signs commonly include vomiting, diarrhea, decreased appetite, weight loss, and lethargy. Signs are usually slowly progressive and poorly responsive to symptomatic therapy. Hematologic findings include anemia and panhypoproteinemia, especially in dogs with diffuse intestinal lymphoma. Lymphoma must be considered in any dog with hypoproteinemia that occurs in conjunction with GI signs (IBD, lymphangiectasia, and histoplasmosis are the main disorders to rule out).
Endoscopy has been very reliable for diagnosing diffuse intestinal lymphoma in dogs in my experience. As opposed to cats, dogs rarely have the nearly pure lymphocytic form of IBD; therefore there are not many cases in which a pathologist will have difficulty in differentiating IBD from lymphoma. However, it is essential that biopsy samples be obtained as deeply in the intestinal mucosa as possible. Proper instrumentation and technique are very important. To maximize my efforts to obtain adequate amounts of tissue for diagnosis, I routinely perform upper and lower GI endoscopy in dogs with hypoproteinemia caused by intestinal disease. After complete colonoscopy, a pediatric endoscope can be advanced through the ileocolic sphincter and into the ileum of most dogs as small as 8 to 10 lb. I have had several dogs in which lymphoma was identified only on biopsy samples of the ileum. If only upper endoscopy had been done on these dogs, the diagnosis would have been missed.
Eight to 10 or more biopsy samples are obtained from each general intestinal region examined. In some patients more samples are obtained, especially if it seems difficult to get adequate-size samples. Every effort is made to provide the pathologist with diagnostic-quality samples. The importance of making the effort to obtain biopsy specimens as deeply as possible cannot be overemphasized. Lymphocytic-plasmacytic inflammation commonly occurs in conjunction with intestinal lymphoma. Specifically, in one report, marked to severe lymphocytic-plasmacytic infiltration was present adjacent to or occasionally distant from the neoplastic foci in 8 of 15 dogs (53%) with primary lymphoma. The junctional region between neoplastic and nonneoplastic tissue was not sharply demarcated, and often an inflamed mucosa overlaid a submucosal lym- phomatous focus.
Exploratory surgery should be considered for dogs with GI signs and concurrent hypoproteinemia in which there is a poor response to treatment of IBD that was diagnosed via endoscopy. It may be that the poor treatment response is due to lymphoma that has not yet been identified.
Treatment involves multiple-agent chemotherapy. Unfortunately, prolonged remission (more than 3 to 4 months) is uncommon in dogs. Occasionally, prolonged remission (8 to 12 months) can be achieved. Clinical experience indicates that dogs with diffuse intestinal lymphoma have a worse prognosis than those with localized disease. Further information can be found in Chapter 11.
More on the topic NEOPLASIA OF THE SMALL INTESTINE:
- Neoplastic diseases of the small intestines
- Smallintestine
- Etiology
- VOMITING
- References
- ENDOSCOPY
- RADIOLOGY OF THE DIGESTIVE SYSTEM
- Lymphoma in Horses
- Alterations in the small intestinal microflora (Small intestinal bacterial overgrowth)
- hepatic AND PANCREATIC NEOPLASIA