Other Infectious Conditions of the Foot
Canaan Whitfield-Cargile
Infections involving the feet of horses, cattle, and other large animal species are common and almost always caused by contamination from the environment gaining access to the soft tissue or bony structures of the foot within the hoof capsule.
Typically the animal has an acute, progressive lameness such that it is almost non-weight bearing on the affected limb or will bear weight on the toe region of the foot but resist putting the heel on the ground. Other clinical signs include increased digital pulse pressure, heat, and sensitivity to hoof tester pressure over the affected area. Regional nerve blocks can be used to localize the lameness to the foot when doubt exists based on physical examination findings. Because the foot is encased in a shell of horny tissue, exudate from an infectious process often accumulates between the soft tissue and the horn. The exudate then spreads or dissects along that plane in the path of least resistance until an outlet is encountered, frequently near the coronary band and bulbs of the heels, where rupture and drainage can occur.Problems Associated With Horseshoe
Nails ("Nail Prick”)
■ History and Clinical Signs Nail prick (“quicking”) refers to penetration of the sensitive hoof structures, usually the sensitive laminae, by a driven horseshoe nail. Similarly, the term hot nail refers to a nail that does not necessarily penetrate the sensitive laminae but may put pressure on those tissues due to inappropriate proximity. The horse will usually react as the farrier drives or clinches the nail by jerking the foot from the farrier. In some cases, blood may appear on the nail or leak from the nail hole. It is important to realize that nail pricks occur for many reasons and are not always caused by a misdirected nail. Poorly made shoes, nails that are too large, poorly placed nail holes, and faulty nails can also result in a nail prick.
Horses with poor hoof quality, thin hoof walls, or flaring hoof walls can be difficult to nail and thus are at greatest risk for nail prick. Fractious horses and young horses not previously shod may lean on the farrier or repeatedly pull the foot from the farrier, making nail driving difficult. Damage from an improperly driven nail can vary from minimal to serious infection, thus clinical signs also vary. Clinical signs include lameness, sensitivity to hoof testers, and increased digital pulses. Some horses will repeatedly stomp the affected foot or paw the ground immediately after shoeing. Others may point the affected limb after shoeing. Lameness may not be apparent immediately after shoeing and may occur days later when the nail hole becomes infected and the trapped pus begins to exert pressure. This delayed onset is especially common when the nail is too close to sensitive laminae but has not penetrated. The horse usually becomes acutely lame and worsens over time unless treated. Some infected nail holes will travel up the lamellae (white line) and create an abscess or soft spot at the hairline of the coronary band. The abscess will be directly aligned with the hoof wall tubules, leading to the infected nail hole, which is an important diagnostic aid.■ Diagnosis Diagnosis of a misdirected nail warrants great diplomacy from the veterinarian, because many owners become unjustifiably upset with the farrier. Hoof tester examination, paying particular attention to pressure over the driven nails, is an essential diagnostic tool to locate the offending nail. Using a hammer to strike the outside hoof wall may also elicit a painful response over the nail, further increasing suspicion of that specific nail. When an abscess occurs days later, it can be very difficult to be certain that the cause of the abscess was a nail prick versus many other reasons. Unless there is irrefutable evidence of the cause of lameness and abscessation being a nail prick, it is advisable to not suggest that as a cause to avoid undue blame being placed on the farrier.
■ Treatment Pricks from nails can be potentially serious and require immediate treatment. If the nail prick is discovered by the farrier at the time of shoeing, the nail is removed. The nail should be examined for moisture or blood. The nail hole can be irrigated with antiseptics (i.e., povidone-iodine [Betadine] solution or hydrogen peroxide). The nail hole is then packed with iodine-soaked cotton and left open. Often the nail is redirected, and no further treatment is needed. If the horse's immunization status is not current, a tetanus vaccine should be given.
If the offending nail cannot be localized or the nail hole is infected, the shoe is removed. Hoof testers are then used to localize the painful nail hole. Frequently the pressure from the hoof testers will cause black, malodorous liquid pus to exit from the hole. The basis of treatment is to establish drainage. The infected nail hole often requires enlargement with a loop hoof knife or curette. Ideally, a cone-shaped hole is made, with the larger opening at the bottom of the hoof to facilitate drainage. The hole is irrigated and/or the entire foot is soaked in an effort to draw out any remaining infection. An important component of treatment is to protect the foot and nail hole from the environment (e.g., mud, dirt) by keeping the foot bandaged between treatment applications. Additional medications are usually unnecessary unless involvement is extensive. Antiinflammatory medications may be beneficial to decrease pain. Once the infection has cleared, the shoe is replaced and the horse can return to previous level of activity.
■ Prognosis Prognosis is usually good provided that minimal damage occurs to vital structures of the foot. Establishing drainage for sepsis is important to avoid potential complications, such as third phalanx osteomyelitis or coffin joint sepsis.
Subsolar Abscess
Subsolar abscess is one of the most common causes of lameness in the horse and cow, but it is relatively rare in sheep and goats.
The vast majority of lameness in cattle is attributed to hoof problems including infection.1,2 Most often, lameness is caused by a hole or crack in the horny sole, which then becomes packed with dirt, and eventually contamination extends to and is trapped within the sensitive soft tissue beneath the sole. Animals that are housed in exceptionally moist or filthy conditions and have inadequate hoof care or overgrown feet or have underlying pathology in either the hoof or systemic conditions are more prone to this problem. For example, a common presenting complaint of horses with keratomas is repetitive subsolar abscessation, and horses with pituitary pars intermedia dysfunction (PPID) often have recurring subsolar abscesses.3,4 Horses taken from a very dry to a very wet environment, and vice versa, also tend to have a higher incidence of sole abscesses, apparently because of the sudden change in the moisture content of the hoof and the resultant cracking of the sole. Cattle with “corkscrew claw” (a hereditary condition) or other growth deformity in the claw are more prone to sole abscess. Puncture wounds or any form of trauma that introduces contamination to the soft tissue of the sole also may result in abscessation.■ History and Clinical Signs Subsolar abscess is a common cause of acute lameness seen in all horses. There is no signalment or breed disposition. Gravel is a lay term describing the assumed etiology in which a piece of gravel migrates proximally from the white line to the coronary band, leaving an infected tract. Subsolar abscesses may originate from a penetrating wound in the white line, a nail hole, or a deep subsolar bruise. Lameness is usually acute and severe (grade 3 to 4 of 5) and may worsen over time until drainage is established. The horse will often point and may not bear full weight on the affected limb. Distal limb swelling often accompanies a subsolar abscess that has not had drainage established. Systemic signs of infection (fever, lethargy) usually are not associated with subsolar abscesses unless deeper structures are involved.
■ Diagnosis Digital pulses are usually increased, and the hoof capsule may radiate heat. A focal painful area can usually

FIG. 38.32 Opened subsolar abscess draining gray and black purulent material.
(but not always) be located with careful hoof tester examination. Careful paring of the sole and frog may be helpful in locating the abscess, but the clinician must be careful not to damage good, healthy tissue while looking for the infection site. Foot poultices and hot-water foot baths will eventually help localize the affected area by softening the horny hoof tissue. Gray or black purulent material will leak from the infected tract (Fig. 38.32). Radiographs are useful to rule out other causes, such as third phalanx and navicular bone fracture. In some cases a gas or fluid pocket can be identified on radiographs.
■ Treatment Treatment is aimed at establishing adequate drainage. If an opening in the tract is present at the solar surface, it should be enlarged just enough for good irrigation and drainage. This may or may not require sedation or peripheral anesthesia of the foot. If pink tissue or blood is encountered, debridement is discontinued. Large holes should be avoided to prevent solar corium protrusion, which can be a painful sequela to overzealous hoof paring. If drainage occurs at the level of the coronary band and solar surface, through- and-through lavage is beneficial. Debridement at the coronary band level should be minimal to prevent iatrogenic coffin joint contamination. Once drainage is established, protecting the opened sole from the environment is recommended and can be accomplished with a foot bandage. Daily lavage and/or foot soaks in warm water with antiseptics and/or salt should be continued until sepsis and inflammation are eliminated. The shoe is replaced when the affected area is dry and cornified. Large areas may require a plastic pad under the shoe for solar protection.
Antibiotics and NSAIDs are rarely needed except in severe cases or if penetration of deeper structures has occurred. The patient's tetanus immunization should be considered and a toxoid administered if needed, as foot abscesses are among the most common causes of tetanus in horses.5 Principles of treating foot abscesses are the same for all large animal species.■ Prognosis Prognosis for simple subsolar abscess is excellent but worsens if complications develop in which deeper structures of the foot become involved.
Deep Penetrating Injuries to the Sole
■ History and Clinical Signs Most animals' environments are filled with sharp objects that can penetrate the sole, causing severe damage to structures deep within the hoof capsule. All puncture wounds should be considered potentially serious, but those involving the solar white line or caudal frog area require special attention because of potential navicular bursa, digital tendon sheath, DDFT, or distal phalanx involvement.
The clinical signs of a penetrating wound to the sole vary with the anatomic structure involved and chronicity of the injury. The animal may show minimal lameness initially at the time of injury but severe lameness once sepsis is established days later.
■ Diagnosis If owners find a foreign body in the bottom of the animal's foot, they should be instructed to leave the object in the foot unless there is danger of further penetration. This facilitates the ability to determine the track of the offending object, as it can be very difficult even to find the puncture wound in some cases following removal of small, sharp objects due to the elastic nature of the hoof structures and collapsing of the penetration site. Once medical attention is sought, if the object is still present then radiographs are used to determine depth of penetration and location of penetration. If the object has been removed, a close examination of the solar surface of the hoof should commence. Systemic sedation and peripheral anesthesia using an abaxial sesamoid nerve block may be needed to thoroughly examine the penetrated equine foot. Regional IV anesthesia (Bier block) using a tourniquet is the method of choice for producing local anesthesia in cattle. A light paring of the sole and frog areas with a hoof knife may reveal a black spot indicating the penetration site. Paring should be performed carefully so that the solar corium is not injured with the hoof knife. If an entry wound is discovered, the foot is scrubbed and prepared for further diagnostic testing. A sterile flexible probe can be gently inserted into the hole and a radiograph taken to determine its depth and direction. The clinician must take care that inadvertent force or horse movement does not cause the probe to penetrate previously unaffected structures. Alternately, a less invasive and preferred method is to catheterize or place a sterile teat cannula into the hole and inject sterile radiopaque material to determine which structures are involved. Recently, advanced imaging modalities, including MRI, have been used to more accurately define the track of penetrating solar injuries.6
If sepsis of the podotrochlear bursa, DIJ, or digital tendon sheath is suspected or cannot be ruled out, synoviocentesis allowing for instillation of sterile saline to assess communication with the wounds and synovial fluid cytologic analysis and culture should be performed. If distal limb swelling is present, arthro- centesis should be delayed until the cellulitis subsides.
■ Treatment Broad-spectrum systemic antibiotics, antiinflammatory medications, and tetanus prophylaxis are administered if penetration of deep hoof structures is suspected. If deemed necessary, antibiotics are initiated, ideally after synovial fluid has been obtained for bacterial culture. Establishment of drainage, copious lavage with sterile ionic fluid, and debridement of all necrotic tissue are indicated. Involvement of the podotrochlear bursa warrants use of navicular bursoscopy and aggressive medical therapy consisting of daily lavage of the bursa under general anesthesia and local treatment using antibiotics instilled within the bursa and regional limb perfusion. Surgical treatment such as the “street nail” procedure, which opens a window through the central frog and DDFT in the bottom of the foot to reach the navicular bursa, is a drastic and aggressive method of therapy not commonly used in favor of a less-invasive bursoscopy approach.
If the DDFT is involved (septic tendinitis), debridement and removal of frayed and infected tendon fibers may be performed on the standing, sedated horse using a tourniquet and peripheral anesthesia or under general anesthesia, depending on horse temperament and owner financial constraints. After debridement, heel elevation with a 4- to 8-degree wedge shoe decreases weight-bearing forces on the DDFT and provides some pain relief.7
Deep penetrating wounds to the sole, especially the solarwhite line junction, can result in infectious osteitis of the distal phalanx. The horse usually presents with a chronic, recurrent draining tract at the coronary band or solar surface and varying degrees of lameness. Infection of the distal phalanx often results from undetected soft tissue infection or dissecting subsolar abscesses. As the bone infection progresses, blood supply to the area is compromised, and the area of avascular bone separates from the parent bone, forming a sequestrum or lytic area that is apparent radiographically (Fig. 38.33). Localized third phalanx septic osteitis and sequestrum formation may not become radiographically evident for weeks after the initial penetration injury.
Debridement and curettage of all soft and necrotic bone can usually be performed in the standing, sedated animal if its temperament permits. The infected bone is usually discolored and soft and should be curetted to healthy bone margins (see Fig. 38.33). Systemic antibiotics may be indicated in some cases, but in most cases postoperative antibiotics can be most easily administered locally via antibiotic-impregnated beads (polymethyl methacrylate or plaster of Paris) for continued antibiotic release at the infected site. Regional limb perfusion with antibiotics is also beneficial in some cases to treat infection locally and prevent extension to surrounding structures. A foot bandage is placed and changed every 1 or 2 days for the initial few weeks. Application of a bar shoe and hospital plate provides solar protection and decreases the labor and cost of daily bandage changes. The remaining care is as described for subsolar abscesses.
In cattle, simple sole abscesses following penetrating injury may heal quite satisfactorily without bandaging. Penetration of bone or synovial structures is managed as described above, although claw amputation is a treatment option in cattle that is not available to horses.8 In cattle, a wooden block on the unaffected claw of the affected foot elevates the affected claw
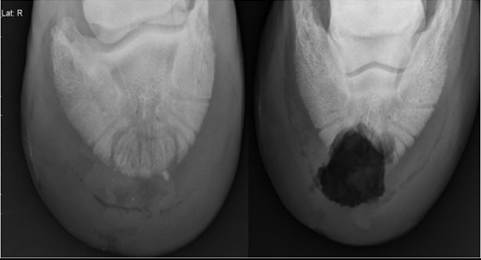
FIG. 38.33 Septic osteitis of the third phalanx before (left image) and after (right image) curettage of the infected region via a solar approach in the standing, sedated horse.
to a non-weight-bearing level and greatly reduces lameness. The block is attached with an epoxy adhesive and allowed to wear off over a period of weeks.
■ Prognosis Prognosis depends on severity of injury, structures involved, and chronicity of the problem before initiating treatment. Overall return to soundness has been reported to range between 36% and 60%, but horses with acute penetrating wounds that receive immediate and aggressive treatment have an excellent prognosis.9,10 Factors that contribute to a poorer prognosis include involvement of a synovial structure, the distal phalanx, and time to presentation to the hospital. Established infection involving the podotrochlear bursa, digital tendon sheath, or distal interphalangeal joint has a poor prognosis.
Prognosis for infectious osteitis of the distal phalanx is good if sepsis is not caused by laminitis.11 In one study, up to 24% of the distal phalanx was removed, and the horse returned to athletic soundness.12
Thrush
■ Definition and Etiology Thrush is a bacterial infection characterized by an accumulation of black, malodorous, necrotic material usually originating within the central or collateral sulci of the frog of the hoof. This degenerative condition may spread to involve deeper structures of the foot, such as the digital cushion, hoof wall, and heel bulb region, causing inflammation and breakdown of these structures.13 This disease in horses is often considered similar to hoof rot in other large animal species.14 Animals standing in soiled stalls, deep mud, swampy land, or wet pastures are at risk for developing thrush. Another predisposing factor is poor hoof conformation. Sad- dlebreds, Tennessee Walkers, and other gaited horses have long feet with naturally deep frog sulci and are at risk of thrush. Horses shod with full pads may develop thrush secondary to moisture and dirt collection under the pad. Other well-kept, clean horses can develop thrush for no apparent reason. Thrush is caused by a bacterial infection that appears to be most commonly associated with Fusobacterium necrophorum; in contrast, foot rot is associated with both F. necrophorum and Dichelobacter nodosus.15
■ Clinical Signs and Diagnosis Lameness may or may not be present, and severity can vary. Diagnosis is based on the presence of black, malodorous discharge, most often within the frog sulci. The central frog sulcus is often malformed and very deep. A painful response may occur when the affected sulci are cleaned because the degenerative process may extend to sensitive structures of the foot. If structural damage has occurred, the heels may move independently of each other, causing pain on manipulation. Horses with mechanical instability of the heels may show caudal heel pain.
■ Treatment The basis for treatment is removing the predisposing cause of the thrush. The horse should be moved to a clean, dry environment and have the feet cleaned daily, and if needed, proper farrier management should be pursued to correct existing problems. Any necrotic debris and undermined tissue are carefully debrided and cleaned using a hoof knife. Foot bandages may be necessary if the debridement is extensive. Infection is usually managed by topical medication. Several caustic materials have been recommended, including a combination of phenol, tincture of iodine and 10% formalin, Kopertox solution, dilute bleach, or methylene blue. Others have recommended soaking the foot in chlorine bleach (1 oz bleach per gallon water). Exercise is important to strengthen the caudal aspect of the foot and will naturally clean the feet. The best prevention for thrush involves educating the client on proper hoof hygiene.
■ Prognosis Prognosis is favorable if the cause of thrush can be identified and eliminated and if the condition is treated before extensive hoof damage has occurred.
White Line Disease (“Seedy Toe”)
■ History and Clinical Signs The white line, visible at the sole, is created by the junction of the insensitive laminae of the hoof wall and the horn of the sole. White line disease has historically described the separation of the hoof wall from its laminar attachments. A crack or opening occurs within the white line, allowing a bacterial or fungal infection to invade the stratum medium close to the laminae, causing cavities to develop between the laminae and the outer hoof wall. Several fungal organisms have been associated with white line disease in horses.16 In environmental conditions with too much moisture (continuous wet pastures) or in drought conditions that produce excessively dry feet, animals are at risk of developing a crack or opening in the white line. Horses with poor-quality hoof walls that split or crack may develop white line disease. In addition, horses with chronic laminitis having a thickened or stretched white line in the toe region (“seedy toe”) are predisposed to this disease.17
The hoof wall separation is usually a chronic condition beginning weeks or months before presentation. Horses with white line disease often show little or no lameness, and therefore the disease is not perceived as an immediate concern by many owners.
■ Diagnosis Visual examination of the white line, assisted by a probing instrument, will reveal a cavity with separation of the outer hoof wall from the laminae. Radiographic evaluation can determine the full extent of hoof wall separation. Often the cavity is either dry or filled with necrotic debris, which may involve a bacterial or fungal infection. The cavity is usually not painful to probing.
■ Treatment Treatment begins with removal of the separated outer hoof wall. After thorough debridement, large defects usually exist in the hoof wall and require protection. A heart-bar shoe redistributes weight-bearing forces to the frog and caudal region of the foot and away from damaged and weakened areas. The hoof wall defects prevent normal nailing procedures, and shoe clips can help secure the shoe to the hoof. After hoof wall removal, the exposed laminae may still have an active infectious component, requiring continued topical application of antiseptics. Once the exposed laminae are dry and inactive, the horse may be a candidate for prosthetic hoof wall repair using an acrylic polymer.
■ Prognosis Prognosis depends on response to treatment and the cause of the original white line problem. Horses with poor hoof quality or seedy toe will often have disease recurrence. If the horse responds to original treatment and if environmental conditions improve, prognosis is good.
Quittor
■ History and Clinical Signs Quittor is a term used to describe chronic infection of the medial or lateral collateral cartilage of the distal phalanx in the horse. This condition is characterized by local inflammation and necrosis of the affected cartilage, with subsequent formation of draining tracts proximal to the coronary band. The infection is usually caused by a wound, and the horse often presents with moderate to severe lameness and a history of chronic or recurrent drainage.
■ Diagnosis The diagnosis is based on clinical signs and radiographic findings. Specifically, obtaining a dorsopalmar radiographic view after injecting contrast dye into the draining tract helps demonstrate the infected collateral cartilage.
■ Treatment Although this condition occasionally responds to medical therapy, the treatment of choice is surgical debridement with the horse under general anesthesia, the foot in full extension, and a tourniquet around the pastern. An elliptical section that includes the draining tract should be incised above the coronary band and discarded. All underlying infected soft tissue and necrotic cartilage should be excised. The incision can be closed, partially closed, or left open to allow for continued debridement if necessary, based on severity of infection and the surgeon's confidence in complete resection of affected tissues. If the condition is chronic with extensive cartilage necrosis or multiple draining tracts, the infectious process usually extends below the level of the coronary band. In these cases it is best to trephine a hole in the hoof wall at the lowest point of the infection. This procedure provides better drainage, facilitates debridement of the necrotic cartilage, and allows for complete closure of the surgical incision above the coronary band. The wound should be packed through the trephine hole and treated as an open wound until it heals. In cases with extensive cartilage necrosis, care should be taken to avoid accidental opening of the coffin joint. If debridement is complete and the distal interphalangeal joint has not been entered during surgery, the prognosis for the return to soundness is fair to good.18
More on the topic Other Infectious Conditions of the Foot:
- Smith Bradford P., Van Metre David C., Pusterla Nicola (eds.). Large Animal Internal Medicine. Part 2. 6th edition. — Elsevier,2020. — 2279 p., 2020
- Clinical Examination for Diagnosis ofWeight Loss
- DISEASES
- Etiologic Diagnoses
- Bacterial Diseases
- Weight Loss
- Nutritional and Metabolic Diseases
- Contagious Ecthyma (Sore Mouth, Orf, Contagious Pustular Dermatitis, Scabby Mouth)
- Environmental Insults
- Cardiac Arrhythmias