stomach tumors in dogs
Background
The most common tumor of the stomach in dogs is gastric adenocarcinoma, which is emphasized in most reports. Leiomyoma, leiomyosarcoma, lymphoma, and adenoma are also found, less commonly.
Most carcinomas occur in the lower two thirds of the stomach, particularly in the pylorus region. The lesser curvature is not usually affected, except in Belgian shepherds. Most affected dogs are old, and there appears to be a male predominance.
Belgian shepherds in Italy (of the Groenendael type) and rough collies are apparently at high risk for gastric adenocarcinoma. Although gastric carcinomas can be experimentally induced in dogs by various compounds, there are no epidemiologic studies to support a role for these compounds in naturally occurring disease.
Gastric leiomyomas are benign tumors of the stomach and are strongly associated with age in the dog.
Clinical Parameters
Gastric tumors are consistently associated with vomiting, weight loss, and inappetence. Vomiting is often chronic and rarely associated with eating. Hematemesis occurs in up to 50% of dogs. Other signs include polydipsia, abdominal pain, melena, and anemia. Occasionally ascites occurs as a result of carcinomatosis. Clinical signs, such as vomiting, are often chronic for 2 weeks to 18 months before presentation; the median duration is 2 months.
There are reports of dogs presenting with metastatic testicular adenocarcinoma, with the primary tumor originating from the stomach.
Leiomyomas are often discovered as incidental findings during necropsy, surgery, or endoscopy in geriatric dogs. Leiomyomas may be identified from a history that reveals chronic vomiting, acute gastric distention, or intermittent severe GI bleeding.
Dogs with gastric leiomyosarcoma may present with clinical signs associated with hypoglycemia, such as weakness, seizures, or coma.
Clinical Work-up
Gastric adenocarcinomas often involve a large area of the stomach wall, making them unresectable. These tumors arise in the mucosa, but most extend to or through the serosa. Ulceration is common and often deep and craterlike, causing hematemesis or melena. Contrast radiography, particularly with fluoroscopy, may give indications of gastric tumor, but these indications are rarely definitive. Endoscopy can determine the location of most tumors, except when neoplasia is diffusely infiltrative, and may reveal tumor ulceration (Figure 11-6).Although endoscopy can be definitive, it can also be inconclusive. Multiple endoscopic biopsy specimens should be obtained, and deep biopsy specimens should be taken if the mucosa is not obviously involved (Figure 11-7). Endoscopy is ideal for evaluating the stomach itself, but ultrasonography should be used to assess epigastric lymph nodes and other abdominal viscera for evidence of metastasis. Ultrasonography or laparoscopy can also be used to define the borders of localized tumors and to identify ulcerations and diffuse infiltration. In one report the use of ultrasonography in the diagnosis of canine gastric neoplasia was evaluated prospectively in a series of six cases that were subsequently confirmed as having adenocarcinoma by cytologic or histologic examination or both. These investigators found that gastric neoplasia was associated with mural thickening, loss of normal wall sonographic layers, and altered motility. Ultrasound findings were consistent with tumor localization obtained by other diagnostic methods that were employed. Fine-needle aspirations of the masses were successful in two out of three cases in which they were performed. Ultrasound-guided microcore biopsy can have a high diagnostic sensitivity. When the aforementioned modalities are unsuitable, exploratory laparotomy or laparoscopy can be used to obtain biopsy specimens from affected sites. A therapeutic excisional biopsy may be possible for small localized tumors via exploratory laparotomy; however, incisional biopsy should be performed on larger tumors.
Gastric adenocarcinoma often metastasizes, particularly to perigastric lymph nodes and viscera. Extension of gastric adenocarcinoma through the serosa creates an intense scirrhous reaction in the mesentery and omentum, which may cause ascites.
Histology of gastric adenocarcinomas varies, and “intestinal” types of tumors (e.g., papillary, aci-

FlGURE 11-6 Endoscopic view of a gastric carcinoma resulting in a mild “cobblestone” effect to the mucosal surface. Note the ulcers in the upper right-hand portion of the image.This dog’s only clinical sign was intermittent vomiting. A partial gastrectomy was performed, and the vomiting and endoscopic abnormalities resolved. (Photo courtesy Dr. David Twedt.) nar, or solid) are less common than diffuse types (e.g., undifferentiated or glandular). No differences in biologic behavior have been ascribed to these different tumor types. All gastric adenocarcinomas are aggressive malignancies.
Therapeutic Approach
The advanced stage of gastric adenocarcinomas at diagnosis, their diffuse nature, and their high rate of metastasis usually make surgery unsuccessful. Most tumors are too large or invasive for complete resection. Wide resection often requires gastro- duodenostomy (Billroth type I procedure); however, most dogs die within 4 months of surgery from local recurrence and metastases. Earlier diagnosis occasionally allows successful surgical resection and long-term freedom from recurrence and metastasis. There is a report of long-term survival after total gastrectomy for gastric adenocarcinoma in a dog. In this dog the esophagus was anastomosed to a remnant of the antrum, leaving the pylorus intact, and a splenopexy was performed. Another long-term survival case is illustrated in Chapter 1 (see pp.22-33).
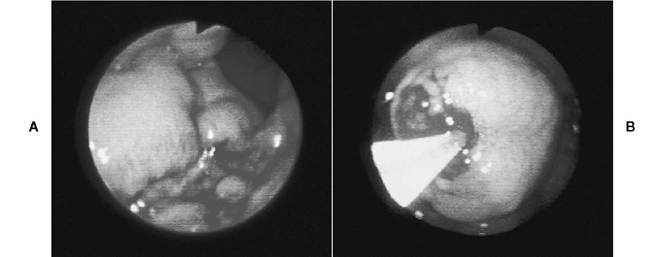
Figure 11-7 Gastric adenocarcinoma in a dog.
A, Lower gastric body with an area of superficial ulceration seen in the lower field. B, Close-up view of a mass in the midgastric bodyThe mass was rigid and had a very dense wall (suggestive of neoplasia). Biopsy of masses such as this one should be performed as deeply as possible. If only superficial tissue is obtained, the endoscopist may fail to retrieve neoplastic cells.The first four attempts to perform a biopsy of the mass yielded very small tissue samples, but on the fifth attempt the biopsy instrument advanced inside the mass. A number of large tissue samples were then obtained, and the diagnosis of adenocarcinoma was confirmed. Biopsy samples were also obtained from the ulcerated area shown in A. (Courtesy Dr. Todd R. Tams. From Tams TR, ed: Small animal endoscopy, ed 2, St. Louis, 1999, Mosby.)Photodynamic therapy with rhodamine dye was not successful in treating an unresectable tumor. Results of chemotherapy for adenocarcinoma have not been reported.
A technique using gastrotomy and submucosal resection was evaluated for removal of leiomyomas and other benign masses from the cardiac region of the stomach. There were no postoperative complications in the six dogs that underwent the procedure, and excision was incomplete in two of the dogs.
More on the topic stomach tumors in dogs:
- stomach tumors in dogs
- intestinal tumors in dogs
- Neoplastic conditions of the stomach
- References
- hepatic AND PANCREATIC NEOPLASIA
- References
- Neoplastic conditions of the liver
- Gastrinoma
- esophageal NEOPLASIA AND PERIESOPHAGEAL MASSES
- Appearance of the upper gastrointestinal tract