Neoplastic conditions of the stomach
Ann B. Hohenhaus
Introduction
Gastric tumors are rare in dogs. Typically, dogs with gastric tumors are older, with a median age of 10 years, but dogs less than 5 years old have also been reported.
A sex predilection has not been consistently reported. Some case series report an equal male to female ratio, but most report a male predominance.1-8 Breed predispositions for gastric tumors include the Chow Chow, Staffordshire Bull terrier, and Rough Collie for gastric carcinoma, and the Belgian Shepherd for mucinous adenocarcinoma of the lesser curvature.1,4,6Tumors can occur in any region of the canine stomach and there does not appear to be an anatomical predisposition for any particular region. One early case series found neoplastic tissue extending into both the body and pylorus of the stomach of most dogs with gastric tumors.7 More recently, the lesser curvature of the stomach has been a frequently described location for gastric tumors.4,8,9 Carcinoma, leiomyoma, and leiomyosarcoma have been found to occur in the pyloric an- trum.2
Gastric tumors are exceedingly rare in cats. Lymphoma, which is a rare gastric tumor in the dog, is the most common gastric tumor in the cat. Three published case series including 96 cats with gastrointestinal tumors report a total of 3 cases of gastric carcinoma.8,10,11 However, age, breed, and sex predilections cannot be determined from such a small number of cases.
Histology
Three major histological types of gastric tumors have been described: carcinomas, sarcomas, and round cell tumors, which are most commonly lymphoma. Although most gastric tumors in dogs are malignant, benign gastric tumors have also been reported.2,9,12,13 Morphologically, carcinomas can be classified as intestinal (also called tubular) or diffuse (Table 4.7).5 The intestinal type of gastric carcinoma can be further differentiated into papillary, acinar, and solid.
Also, the diffuse type of gastric carcinoma can be further differentiated into adenocarcinoma (glandular carcinoma) and the undifferentiated carcinoma. Signet ring cells containing mucin are characteristic of undifferentiated carcinomas. The scirrhous nature of gastric carcinomas is the result of desmoplasia induced by the malignant epithelium. Both types of diffuse carcinomas show desmoplasia, while intestinal type gastric carcinomas tend to be less scirrhous. A gastric carcinoid tumor has been reported in both a dog and a cat.14,15Table 4.7: Histological types of gastric carcinoma
Subtype Form
Intestinal (tubular) type ■ Acinar
■ Papillary
■ Solid
Diffuse type ■ Adenocarcinoma
■ Undifferentiated carcinoma (signet ring)
Clinical signs
The clinical signs of gastric neoplasia are similar to those seen with other gastric disorders.Vomiting is common and in many cases is due to gastric outflow obstruction. Malignant ulceration occurs in more than 50% of dogs with a gastric carcinoma (Figure 4.18). Hematemesis, melena, and pallor due to anemia are also commonly seen.5,7 Tumor-associated nausea can be responsible for anorexia, weight loss, cachexia, and ptyalism.
Clinical pathology
The results of clinical pathology testing are not specific for gastric tumors in general or for a specific histological type of gastric neoplasia. Clinicopathological abnormalities are, in general, due to gastric inflammation, gastric outflow obstruction, malabsorption, or blood loss. Hypoproteinemia and elevated liver enzymes are common.1,3 In dogs with tumor- induced gastric outflow obstruction and vomiting, a hypochloremic metabolic alkalosis with paradoxical aciduria may develop.3 Frequently, a CBC demonstrates an inflammatory leukogram and anemia.1,3 If the gastric bleeding is acute, the ensuing anemia will be regenerative, but if the hemorrhage is chronic, the anemia will become non-regenerative.
Diagnostic imaging
Diagnostic imaging is extremely important in determining the presence of a gastric mass and the extent of involvement of the surrounding organs. Unfortunately, the features of both benign and malignant gastric masses as well as the various histological types of gastric neoplasia overlap and neither abdominal radiography nor abdominal ultrasonography are useful in differentiating the specific tumor types.
Radiography
In some patients with gastric tumors, the survey radiographs may be normal. Abnormal findings include excessive fluid or gas in the stomach despite fasting.3 A mass or caudal displacement of the gastric axis on the lateral radiograph has been described in dogs with gastric tumors.2
The use of contrast agents facilitates the radiographic visualization of gastric wall thickening, distortion of the gastric lumen, presence of a filling defect, and derangement of the rugal folds caused by tumor infiltration. While the normal gastric emptying time is not well defined, delayed emptying is common with gastric tumors.2,3 The stomach may also appear rigid and non-distensible, which is termed “linitis plastica” or “leather bottle stomach”. Ulcers can also be highlighted by contrast material.7
Ultrasonography
Both benign and malignant gastric tumors can be associated with mural thickening, loss of normal wall layering, and decreased or absent motility in the area of the tumor.1,3,12,16 The echogenicity of gastric tumors may be hypoechoic, hypere- choic, or mixed regardless of the histologic type.12,16 Carcinomas and lymphomas may appear as sessile masses or diffuse in distribution, while leiomyomas and leiomyosarcomas are typically focal in distribution.12 An ultrasound finding termed pseudolayering appears to correlate with an uneven intramural distribution of tumor cells seen histologically in dogs with gastric carcinoma.1 Extension of the tumor through the serosal surface of the stomach has been identified in dogs with carcinoma.12
The accuracy of ultrasonography increases with the expertise of the ultrasonographer.
The utility of ultrasound in identifying gastric masses is decreased when the patient is uncooperative or gas and ingesta obscure the stomach wall. In addition, non-neoplastic gastric disorders such as gastritis can appear identical to gastric neoplasia in some cases.9 Ultrasonography is also useful to identify regional lymphadenopathy; although finding enlarged lymph nodes is not specific for metastatic gastric neoplasia.Biopsy techniques
Although clinical signs, laboratory data, and diagnostic imaging may be suggestive of a gastric tumor, a biopsy is essential for a definitive diagnosis. Exploratory laparotomy can be used to obtain tissue samples for biopsy. Multiple samples can easily be obtained and are typically adequate in size for arriving at an accurate diagnosis, but the procedure is invasive. Gastroscopy, using a fiberoptic or video endoscope, allows collection of a tissue sample and visualization of the gastric lesion prior
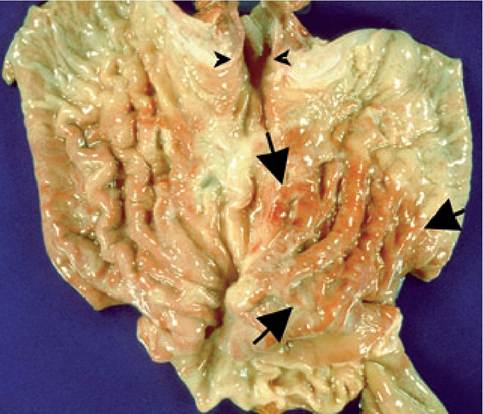
Figure 4.18:
Gastric adenocarcinoma in a dog. The arrows mark the outline of a gastric adenocarcinoma. The entrance of the esophagus into the stomach is shown by the arrowheads.
to any therapeutic surgical procedure. Samples tend to be small and 10-20% of samples may be inadequate for obtaining an accurate diagnosis. Ultrasound-guided percutaneous fine needle aspiration of gastric masses to obtain cytologic samples has been reported; and this procedure appears to be useful for the diagnosis of gastric tumors in some patients.1,3,17
Treatment
Because gastric tumors are rare and, in many cases, advanced at the time of diagnosis, reports of treatment are limited to single case reports. Surgery has been the primary treatment modality used in most cases. A relief of gastric outflow obstruction by side-to-side gastrojejunostomy has been achieved.2 Total gastrectomy or gastroduodenostomy have been attempted to achieve complete tumor resection.2,18 One dog undergoing gastroduodenostomy was provided nutrition through a jejunostomy tube and was also treated with chemotherapy using a combination of cisplatin, 5-fluorouracil, doxorubicin, and cyclophosphamide.2 Photodynamic therapy has also been reported for the treatment of a gastric carcinoma in a single case.4
Systemic complications of gastric neoplasia
Hypochloremic metabolic alkalosis resulting in paradoxical aciduria occurs in dogs with gastric carcinoma and severe vomiting.3 Vomiting leads to the loss of hydrogen and chloride
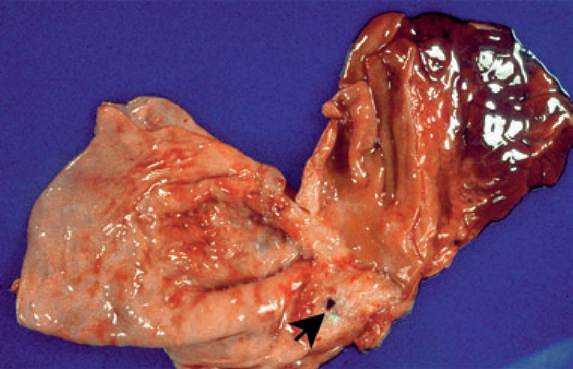
Figure 4.19:
Gastric perforation in a dog with gastric adenocarcinoma.
The arrow points to a gastric perforation as a result of a gastric adenocarcinoma in a dog.ions, alkalosis, and volume depletion. Normally, the renal tubules will resorb sodium ions in exchange for chloride ions in response to alkalosis and hypovolemia. However, when chloride is depleted, the kidneys resorb sodium and excrete hydrogen ions instead of chloride in order to maintain electrical neutrality, leading to a paradoxical aciduria.
Iron deficiency anemia results when gastric tumors cause ulceration and chronic GI blood loss. Loss of iron into the feces and inadequate intake of replacement iron due to vomiting and anorexia result in a microcytic, hypochromic, non-regen- erative anemia.
Paraneoplastic hypoglycemia with a low serum insulin concentration has been described in a dog with a gastric leiomy- osarcoma.19 The diagnostic investigation of this patient suggested the synthesis of an unidentified hypoglycemic factor by the tumor. Non-islet cell tumors associated with hypoglycemia such as this one are typically large and palpable on physical examination.19 Pneumoperitoneum results when the tumor erodes through the entire gastric wall (Figure 4.19).20
Tumor invasion and metastasis
All histological types of gastric tumors are highly metastatic. Gastric carcinomas most commonly metastasize to the regional lymph nodes, but they can also widely disseminate to other abdominal organs, the central nervous system, the myocardium, mediastinum, long bones, and testicular connective tissue.2,4,16,21,22 The single case of a gastric carcinoid tumor in a cat was found to have metastasized to the kidney, brain, liver, spleen, lung, and lymph node.11 Gastric leiomyosarcomas have been shown to metastasize to the liver and duodenum 2.
Survival
In general, the survival of dogs with gastric cancer is poor. One case series reported a median survival time of 3 days with a range of 0 days to 10 months.2 Occasionally, longer survival times have been reported in single cases.
Survivals of 240 days and 9 months were reported in two dogs undergoing gastrectomy.18,23??Θ Key Facts
■ Most gastric tumors are malignant and are highly metastatic.
■ Diagnostic imaging, plain radiography, contrast radiography, and ultrasonography contribute to the diagnosis of gastric tumors; however, a biopsy is required to make a definitive diagnosis and to determine if the tumor is benign or malignant.
■ Tissue samples can be obtained via exploratory laparotomy or endoscopy.
■ Between 10-20% of the time, a sample obtained via endoscopy will be inadequate to diagnose gastric cancer.
■ In general, survival in dogs and cats with gastric neoplasia is poor due to the advanced stage of disease at the time of diagnosis.
References
1. Penninck DG, Moore AS, Gliatto J. Ultrasonography of canine gastric epithelial neoplasia. Vet Radiol Ultrasound 1998; 39: 342— 348.
2. Swann HM, Holt DE. Canine gastric adenocarcinoma and leiomyosarcoma: a retrospective study of 21 cases (1986—1999) and literature review.JAm Anim Hosp Assoc 2002; 38: 157—164.
3. Rivers BJ, Walter PA, Johnston GR et al. Canine gastric neoplasia: utility of ultrasonography in diagnosis. J Am Anim Hosp Assoc 1997; 33:144-155.
4. Fonda D, Gualtieri M, Scanziani E. Gastric carcinoma in the dog: a Hinicopathological study of 11 cases. JAm Small Anim Prac 1989; 30: 353-360.
5. Patnaik AK, Hurvitz AI, Johnson GF. Canine gastric adenocarcinoma. Vet Pathol 1978; 15: 600-607.
6. Sullivan M, Lee R, Fisher EW et al. A study of 31 cases of gastric carcinoma in dogs. Vet Rec 1987; 120: 79-83.
17. Sautter JH, Hanlon GF. Gastric neoplasms in the dog: a report of 20 cases. JAm Vet Med Assoc 1975; 166: 691-696.
18. Gualtieri M, Monzeglio MG, Scanziani E. Gastric neoplasia. Vet Clin North Am 1999; 29: 415-440.
9. Easton S. A retrospective study into the effects of operator experience on the accuracy of ultrasound in the diagnosis of gastric neoplasia in dogs. Vet Radiol Ultrasound 2001; 42: 47-50.
10. Brodey RS. Alimentary tract neoplasms in the cat: a clinicopatho- logic survey of 46 cases. Am J Vet Res 1966; 27: 74-80.
11. Turk MAM, Gallina AM, Russell TS. Nonhematopoietic gastrointestinal neoplasia in cats: a retrospective study of 44 cases. Vet Pathol 1981; 18: 614-620.
12. Lamb CR, Grierson J. Ultrasonographic appearance of primary gastric neoplasia in 21 dogs. J Small Anim Prac 1999; 40: 211-215.
13. Kapatkin AS, Mullen HS, Matthiesen DT et al. Leiomyosarcoma in dogs: 44 cases (1983-1988). J Am Vet Med Assoc 1992; 201: 10771079.
14. Albers TM, Alroy J, McDonnell JJ. A poorly differentiated gastric carcinoid in a dog.J Vet Diagn Invest 1998; 10: 116-118.
15. Rossmeisl JH, Forrester SD, Tobertson JL et al. Chronic vomiting associated with a gastric carcinoid in a cat. J Am Anim Hosp Assoc 2002; 38: 61-66.
16. Kaser-Hotz B, Hauser B, Arnold P. Ultrasonographic findings in canine gastric neoplasia in 13 patients. Vet Radiol Ultrasound 1996; 37: 51-56.
17. Crystal MA, Penninck DG, Matz ME et al. Use of ultrasound-guided fine-needle aspiration biopsy and automated core biopsy for the diagnosis of gastrointestinal diseases in small animals. Vet Radiol Ultrasound 1993; 34: 438-444.
18. Sellon RK, Bissonnette K, Bunch SE. Long-term survival after total gastrectomy for gastric adenocarcinoma in a dog. J Vet Intern Med 1996; 10: 333-335.
19. Bellah JR, Ginn PE. Gastric leiomyosarcoma associated with hypoglycemia in a dog. JAm Anim Hosp Assoc 1996; 32: 283-286.
20. Mellanby RJ, Baines EA, Herrtage ME. Spontaneous pneumoperitoneum in two cats. J Small Anim Pract 2002; 43: 543-546.
21. Esplin DG, Wilson SR. Gastrointestinal adenocarcinomas metastatic to the testes and associated structures in three dogs.J Am Anim Hosp Assoc 1998; 34: 287-290.
22. Wang FI, Lee JJ, Liu CH et al. Scirrhous gastric carcinoma with mediastinal invasion in a dog.J Vet Diagn Invest 2002; 14: 65-68.
23. Beck C, Slocombe RF, O’Neill T et al. The use of ultrasound in the investigation of gastric carcinoma in a dog. Aust Vet J 2001; 79: 332334.
5
More on the topic Neoplastic conditions of the stomach:
- Neoplastic conditions of the stomach
- Indications
- Stomach
- Neoplastic conditions of the liver
- Smallintestine
- Steiner J.M. (ed.). Small Animal Gastroenterology. Schluetersche,2008. — 387 p., 2008
- Liver and biliary tract
- Diagnostic approach to patients with suspected liver disease
- References
- Subject Index