Urinary System Disorders in the Foal
Thomas J. Divers • Dominic R. Dawson-Soto • Lisa E. Fultz
Umbilical disorders of the neonatal foal, including patent urachus, urachal infections, and omphalitis, are discussed in detail in Chapter 17.
Uroperitoneum
BLADDER RUPTURE. The most common bladder disorder in otherwise healthy newborn foals is bladder rupture.1-3 Foals aged less than 1 week are the most commonly affected, with an incidence of 0.2% to 2.5%.4 There may be an increased incidence in colts, but some reports fail to support this.4,5 In septic foals, bladder necrosis leading to leakage of urine may occur, possibly secondary to hematogenous spread of bacteria.6 E. coli was the most common bacteria isolated from both peripheral blood and tissue sample in septic foals with ruptured bladders.4 Focal necrotizing cystitis leading to tiny focal bladder perforations, uroperitoneum, and peritonitis has been reported in association with septic omphalitis in a 15-day-old foal, and Clostridium perfringens urachal infection was identified as a cause of uroperitoneum in two neonatal foals.7,8 Clinical signs include stranguria and repeated posturing to urinate during the first few days of life. Urine accumulates in the abdomen, typically leading to depression and abdominal distention between days 2 to 4 of life. Repeated posturing and stranguria can easily be misinterpreted as tenesmus associated with meconium impaction. Further, affected foals may continue to void small volumes of urine, so establishing a diagnosis of ruptured bladder can initially be challenging until more obvious signs of uroperitoneum (e.g., decreased nursing, abdominal distention) develop.
Laboratory findings in foals with uroperitoneum include i "i Ii "i ιi" i ∙ 13 9 10
hyponatremia, hypochloremia, hyperkalemia, and azotemia.13,9,10 Foals receiving continuous fluid therapy before the diagnosis may not exhibit typical electrolyte changes, and instead suspicion of uroperitoneum should be raised with other signs such as decreased urinary output, abdominal distention, weakness, or other changes in clinical condition.
Occasionally, a foal may also develop intermittent fine muscle tremors or a cardiac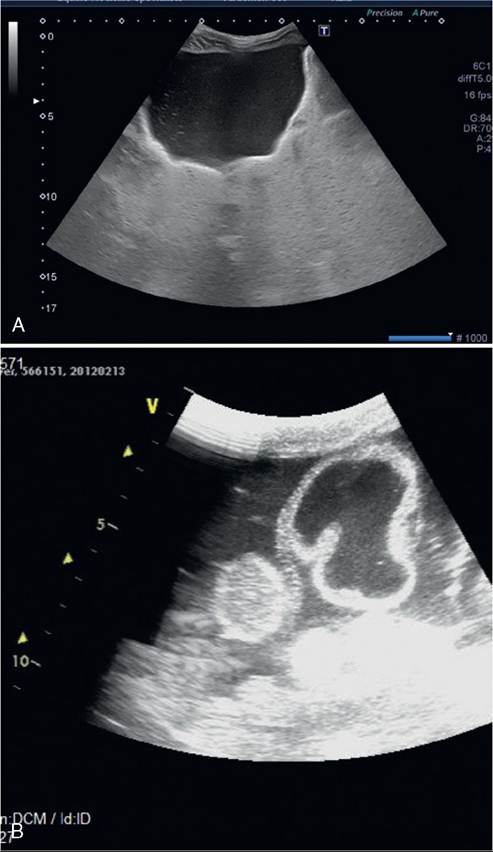
FIG. 34.15 A, Ultrasonographic appearance of a normal bladder in a foal. B, Ultrasonographic image of a ruptured bladder in a foal. The increased free peritoneal fluid is outlining the bladder and a loop of small intestine. The creatinine within the fluid was greater than twice that of the serum, consistent with uroabdomen.
arrhythmia resulting from these electrolyte alterations, especially hyperkalemia.10 Transabdominal ultrasonographic examination usually reveals a large quantity of free fluid in the abdominal cavity, but occasionally the bladder can still appear fluid filled, depending on the size of the leak (Fig. 34.15, A and B). A peritoneal fluid creatinine-to-serum creatinine ratio >2 : 1 or the presence of calcium carbonate crystals in the abdominal fluid confirms uroperitoneum.1-3,9
Treatment of bladder rupture includes surgical closure of the defect, supportive care, and broad-spectrum prophylactic antibiotics for 3 to 7 days postoperatively.1,2,6,11 An emergency surgical procedure is usually not required, and in most cases, postponement of surgery for several hours until electrolyte abnormalities are partially corrected (most notably correction of hyperkalemia to a serum concentration 2 kg in 24 hours) is another common finding in hospitalized neonates that develop uroperitoneum, along with decreased urinary output. Transabdominal ultrasonography can be useful in detecting inappropriate urachal patency and communication with the bladder (Fig. 34.16, A and B).
Laboratory abnormalities typical for uroperitoneum may be found in affected foals but are not consistently abnormal, because these patients are often being treated with IV fluids. Correction of the problem includes surgical removal of the diseased urachus, closure of the bladder apex, and continued supportive care for the primary disease.
The prognosis for a successful outcome for these foals is not as favorable as for bladder rupture because they often have a degree of peritonitis (increasing risk for adhesions), and uroperitoneum is often only one of several complications of the underlying disease.4,11In an occasional foal, the urachus may also rupture more distally than usual and lead to subcutaneous accumulation of urine, ventral abdominal swelling, stranguria, signs of colic, and distress.14 The swelling may be differentiated clinically from a hematoma or septic omphalitis because it may enlarge quickly and often becomes cold. Ultrasonographic examination and/or local aspiration of fluid and measurement of creatinine (twofold or greater than in serum) confirm the diagnosis. Prompt surgical removal of the leaking urachus is indicated.
URETERAL DEFECTS. Ureteral defect(s) or disruption may also lead to development of uroperitoneum in both male and female foals.1 Although rare in comparison with bladder rupture in foals, numerous case reports do exist, encompassing both traumatic and congenital ureteral abnormalities.15-23 Stranguria is usually absent, and urine initially accumulates in the
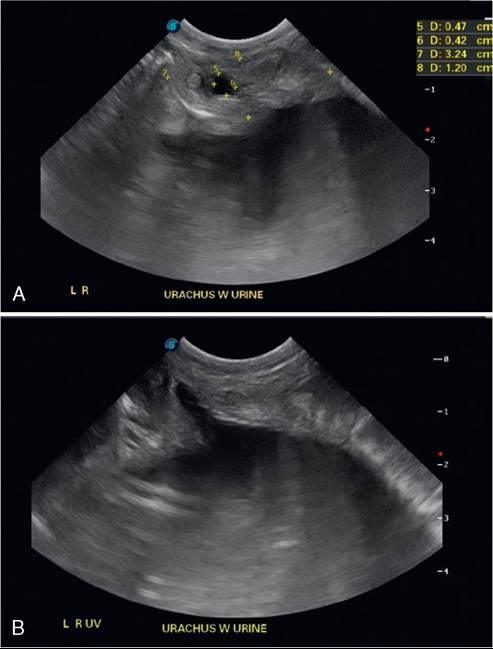
FIG. 34.16 A, Ultrasonographic image of hypoechoic fluid within a foal’s urachal remnant, consistent with patent urachus. B, Ultrasonographic image of communication between the urachus and bladder in a foal, diagnostic of patent urachus.
retroperitoneal space, but with time the retroperitoneal tissue ruptures, causing uroperitoneum. Affected foals may not be presented until 5 to 10 days of age or even older because urine accumulation is slower than with a ruptured bladder. Clinical signs include decreased nursing, depression, and mild colic, and in fillies an external bulging of the vagina may be observed. Laboratory findings are typical for uroperitoneum, and with significant hyperkalemia, intermittent muscle fasciculations may also be noted.
If urine accumulation remains localized to the retroperitoneal space, ultrasonographic examination of the lower abdomen may be normal, but a large amount of retroperitoneal fluid will be detected around the kidney and upper flank (within retroperitoneal space) on the affected side(s). In addition, the renal pelvis may be mildly dilated.24 If the peritoneal membrane is ruptured, physical and ultrasonographic examination findings are similar to those seen with a ruptured bladder, but careful ultrasonographic examination may also reveal a full bladder or concurrent retroperitoneal fluid accumulation. As with a ruptured bladder, the ratio of retroperitoneal or peritoneal fluid creatinine-to-serum creatinine is >2:1. In small foals (e.g., or both ureters may be involved, and during surgical exploration, one or more defects can usually be found in the proximal half of the ureter, often near the renal pelvis. During surgery the defect(s) can be localized by Catheterizing the ureter through a cystotomy and then injecting dye (e.g., Evans blue, methylene blue). Successful correction of unilateral and bilateral defects can be accomplished by placing a stent in the affected ureter(s) for 7 to 26 days.15,16,23 Surgical reimplantation of a ureter into the bladder (ureteroneocystostomy) has also been used to successfully correct a stenotic ureter in a 2-day-old foal.23
A report describing bilateral ureteral defects adjacent to the renal pelves provided histopathologic evidence that the lesions were traumatic in origin rather than developmental anomalies.18 The foal in that report had previously been kicked by its dam. One of the authors (TJD) has seen three foals with similar ureteral defects, all of which also had multiple rib fractures. Ureteropelvic junction injuries and proximal ureteral tears are a recognized complication after blunt abdominal trauma in human patients.25 These observations suggest that many ureteral defects in foals may more likely be traumatically induced at foaling rather than being developmental anomalies.
However, there are several case reports of nontraumatic congenital ureteral defects in foals.17,20,21,23Cystitis
Cystitis can develop in septic, recumbent, premature, or neonatal foals being treated with broad-spectrum antibiotics. Evidence indicates that bacterial infection of the urinary tract, whether primary or due to hematogenous spread, may contribute to the development of uroperitoneum.5,6 When cystitis is suspected, the bladder should be catheterized and a urine sample submitted for urinalysis and quantitative culture. Urinary tract infections with Candida spp. are fairly common in recumbent neonates on broad-spectrum antibacterials. Specific antimicrobial therapy is not usually necessary for Candida cystitis as long as systemic antibiotics can be discontinued. However, fluconazole is an option for treatment because if antibiotic therapy continues, dissemination of the Candida infection can sometimes spread to other sites (e.g., joints).
■
More on the topic Urinary System Disorders in the Foal:
- Urinary System Disorders in the Foal
- Smith Bradford P., Van Metre David C., Pusterla Nicola (eds.). Large Animal Internal Medicine. Part 2. 6th edition. — Elsevier,2020. — 2279 p., 2020
- Diarrhea in Neonatal Foals
- Immunosuppression Associated With Immune-Mediated Disorders
- Acute Renal Failure
- REFERENCES
- Motor Unit and Cauda Equina Diseases
- INDEX
- Submission of Laboratory Samples
- Urinary Incontinence