Ocular Neoplasia*
Caroline M. Betbeze • Meredith L. Voyles
A wide variety of tumor types may involve the ocular or periocular tissues of food animals and horses. Except for the most common neoplasms, limited information is available regarding treatment modalities, drug dosages, overall prognosis, and prevention or control.
The tendency has been to adapt information and methods used in other areas of medicine for use in large animals. Table 39.4 lists potential presenting signs and corresponding ocular neoplastic conditions or related differential diagnoses for horses, cattle, sheep, and goats. Table 39.5 categorizes ocular neoplasms that have been reported in the literature for each of these species. The greatest amount of information pertains to the horse.Despite the variety of primary and secondary neoplasms affecting the ocular and periocular tissues, most tumors produce similar effects on the eye, with tissue distortion and loss of function being the initial concerns. Strategic therapy and management goals may vary from curative or palliative (e.g., eliminating discomfort by enucleation) for individuals to elimination of the problem (e.g., culling from the herd) for a population. Tumor treatment options are often similar for neoplasms involving a particular ocular region or location. When designing a management plan, however, the specific histologic tumor type is important in determining prognosis. Classification of a tumor as “benign” versus “malignant” or “localized” (e.g., equine sarcoid) versus “systemic” (e.g., lymphosarcoma) greatly influences treatment options and management approaches. The following discussion addresses the major tumors of concern in large animals and briefly surveys miscellaneous tumors that have been associated with ocular signs.
Bovine Ocular Squamous Cell Carcinoma
■ Definition and Etiology Bovine ocular squamous cell carcinoma (OSCC), commonly called “cancer eye,” represents the most economically important neoplasm of cattle.
It is the most common tumor affecting cattle in North America, and according to estimates from federally inspected abattoirs in the United States, 12.5% of all bovine carcass condemnations were caused by OSCC.1 The economic impact includes carcass condemnations, production losses, treatment expenditures, and management costs.OSCC arises from the epithelial surfaces of the conjunctiva (corneoscleral junction, nictitating membrane, and palpebra) or cornea. The etiology is probably multifactorial, with genetic, environmental, and viral factors being proved or suspected.1-3 In particular, increasing levels of solar irradiation and decreasing amounts of circumocular pigmentation are linked to an increased prevalence of OSCC.4,5
■ Clinical Signs and Differential Diagnoses The gross appearance depends not only on the anatomic tumor site (because this determines the overall interaction between epithelium and underlying connective tissue elements) but also on the stage of malignancy. In general, premalignant squamous cell tumors are small, white, superficial, and elevated hyperplastic plaques or papilloma-like structures with verrucous surfaces (Fig. 39.19). In contrast, malignant tumors are
^Contributions to previous editions by Steven M. Roberts are acknowledged.
■ TABLE 39.4
Ocular Neoplasia and Differential Diagnoses by Species Based on Presenting Clinical Signs
| Clinical Sign | Equine | Bovine | Caprine | Ovine |
| Ocular pain | Habronema blepharoconjunctivitisa Brainstem neoplasia Ocular dermoid Ocular trauma Squamous cell carcinomaa Sarcoid | Brainstem neoplasia Ocular dermoid Orbital lymphosarcomaa Sporadic bovine leukosis Squamous cell carcinomaa | Brainstem neoplasia Ocular dermoid Squamous cell carcinoma | Brainstem neoplasia Ocular dermoid Squamous cell carcinoma |
| Exophthalmos | 1 Optic nerve neuroepithelial tumor 2 Lymphosarcoma 3 Retrobulbar neoplasia | 4 Enzootic adult lymphosarcomaa 5 Nasal and paranasal sinus neoplasia 6 Nonprogressive bilateral exophthalmos 7 Oral, maxillary, and mandibular neoplasia 8 Retrobulbar neoplasia 9 Sporadic bovine leucosis Squamous cell carcinomaa | Nasal and paranasal sinus neoplasia Oral, maxillary, and mandibular neophasia Squamous cell carcinoma | Adenocarcinoma of nasal cavity Nasal and paranasal sinus neoplasia Squamous cell carcinoma |
| Intraocular | Exudative optic neuritis | Ectopic lacrimal gland | Ocular trauma | Ocular trauma |
| mass | Mastocytoma Medulloepithelioma Ocular melanoma Optic disk astrocytoma Optic nerve neuroepithelial tumor Squamous cell carcinoma Proliferative optic neuropathy Uveal or iris cyst | Ocular melanoma Squamous cell carcinoma | Squamous cell carcinoma | Squamous cell carcinoma |
| Nictitating | 10 Horner’s syndrome | 14 Horner’s syndrome | 18 Ocular trauma | 20 Ocular trauma |
| membrane | 11 Ocular trauma | 15 Lymphosarcoma | 19 Nasal and paranasal | 21 Nasal and paranasal |
| protrusion | 12 Orbital neoplasia 13 Nasal and paranasal sinus neoplasia | 16 Ocular trauma 17 Nasal and paranasal sinus neoplasia | sinus neoplasia | sinus neoplasia |
| Nasolacrimal | Cutaneous squamous cell | 23 Nasolacrimal duct | 25 Nasolacrimal duct | 27 Nasolacrimal duct |
| duct | carcinomaa | occlusion | occlusion | occlusion |
| obstruction | Habronema blepharoconjunctivitis 22 Nasal and paranasal sinus neoplasia | 24 Nasal and paranasal sinus neoplasia | 26 Nasal and paranasal sinus neoplasia | 28 Nasal and paranasal sinus neoplasia |
| Ocular | 29 Conjunctivitis | 33 Conjunctivitis | 37 Conjunctivitis | 40 Conjunctivitis |
| discharge | 30 Ocular trauma 31 Lymphosarcoma 32 Nasal and paranasal sinus neoplasia Retrobulbar neoplasia | 34 Ocular trauma 35 Lymphosarcoma 36 Nasal and paranasal sinus neoplasia Retrobulbar neoplasia | 38 Lymphosarcoma 39 Nasal and paranasal sinus neoplasia | 41 Lymphosarcoma 42 Nasal and paranasal sinus neoplasia |
| Periorbital or | 43 Adenocarcinoma | 55 Ectopic lacrimal gland | 62 Fibroma | 66 Fibroma |
| eyeball | 44 Angiosarcoma | 56 Fibroma | 63 Fibrosarcoma | 67 Fibrosarcoma |
| mass | 45 Hemangioma 46 Hemangiosarcoma 47 Lipoma 48 Lymphosarcoma 49 Mastocytoma 50 Melanoma 51 Nasal and paranasal sinus neoplasia 52 Ocular dermoid 53 Reticulum cell sarcoma 54 Retrobulbar neoplasia Sarcoida Squamous cell carcinomaa Warts | 57 Fibrosarcoma 58 Ocular dermoid 59 Ocular melanoma 60 Retrobulbar neoplasia 61 Squamous cell carcinomaa | 64 Melanoma 65 Nasal and paranasal sinus neoplasia Ocular dermoid Papillomatosis Squamous cell carcinoma | 68 Melanoma 69 Nasal and paranasal sinus neoplasia Ocular dermoid Papillomatosis Squamous cell carcinoma |
Continued
■ TABLE 39.4
Ocular Neoplasia and Differential Diagnoses by Species Based on Presenting Clinical Signs—cont'd
| Clinical Sign | Equine | Bovine | Caprine | Ovine |
| 70 Glaucoma 71 Ocular melanoma 72 Ocular trauma 73 Medulloepithelioma Infectious bovine keratoconjunctivitisa Ocular melanoma Ocular trauma | 74 Ocular trauma 75 Ocular melanoma | |||
| Corneal mass | Angiosarcoma | Enzootic adult | Keratomycosis | Keratomycosis |
| Hemangioma | lymphosarcoma | Ocular dermoid | Ocular dermoid | |
| Hemangiosarcoma | Infectious bovine | Squamous cell | Squamous cell | |
| Keratomycosis Ocular dermoid Squamous cell carcinomaa | keratoconjunctivitisa Interstitial keratitis Ocular dermoid Squamous cell carcinomaa | carcinoma Fibroma | carcinoma | |
| Facial mass | Angiosarcoma Cutaneous habronemiasis Hemangioma Hemangiosarcoma Lymphosarcoma Mastocytoma Nasal and paranasal sinus neoplasia Ocular dermoid Ocular melanoma Oral, mandibular, and maxillary neoplasia Retrobulbar neoplasia Salivary gland neoplasia Sarcoida Schwannoma of eyelids Sialoadenitis | Enzootic adult lymphosarcoma Fibroma Melanoma Nasal and paranasal sinus neoplasia Ocular dermoid Ocular melanoma Papillomatosis Retrobulbar neoplasia Sebaceous cyst Sporadic bovine leukosis Squamous cell carcinomaa | Fibrosarcoma Histiocytoma Melanoma Nasal and paranasal sinus neoplasia Papillomatosis Squamous cell carcinoma Fibroma Fibrosarcoma Lymphosarcoma Nasal and paranasal sinus neoplasia Ocular melanoma Papillomatosis Squamous cell carcinoma |
aDenotes the most prevalent and important differential diagnostic considerations.
■ TABLE 39.5
Ocular Neoplasms Reported in Large Animal Species
| Neoplasm | Equine | Bovine | Caprine | Ovine |
| Adenocarcinoma | + | + | ||
| Angiosarcoma | + | |||
| Basal cell tumor | + | |||
| Chondroma rodens | + | |||
| Equine sarcoid | + | |||
| Hemangioma | + | |||
| Lymphangioma | + | |||
| Lymphosarcoma | + | + | + | + |
| Mastocytoma | + | + | + | + |
| Medulloepithelioma | + | |||
| Nasal/paranasal | + | + | ||
| sinus neoplasia | ||||
| Ocular melanoma | + | |||
| Optic nerve | + | |||
| astrocytoma | ||||
| Optic nerve | + | + | ||
| neuroepithelioma | ||||
| Papilloma | + | |||
| Retrobulbar | + | |||
| neoplasia | ||||
| Reticulum cell | + | + | + | + |
| sarcoma | ||||
| Schwannoma | + | |||
| Squamous cell | + | + | + | + |
| carcinoma |
more irregular, nodular, pink, erosive, and invasive in nature (Fig.
39.20). Malignant tumors with accompanying necrosis often have a characteristic foul odor (see Fig. 39.20). Squamous cell carcinomas that invade the orbit may become extensive and eventually invade bone. Often the gross appearance allows a diagnosis to be established, but at times histology is necessary to differentiate among benign tumors, carcinoma in situ, and invasive SCC. Bovine OSCC typically involves (in decreasing order of frequency) the lateral limbus, eyelid margins (especially the lower), nictitating membrane, and medial canthal regions.1,2 (See Color Plate 39.12) Clinical signs resulting from metastatic lesions are not common, although regional lymph nodes may become infiltrated with neoplastic cells.Despite the characteristic appearance of lesions, differential considerations include conjunctival follicular hyperplasia, dermoid, fibroma, fibrosarcoma, granulation tissue, infectious bovine keratoconjunctivitis, lymphosarcoma, and mastocytoma (see Tables 39.4 and 39.5).
■ Pathophysiology The tumor in all species develops through a series of premalignant stages (i.e., hyperplastic plaques or epidermal plaques and papillomas) to progress over months and years to a carcinoma in situ and finally to an invasive squamous cell carcinoma. Neoplastic lesions may arise without notable precursor stages. It is unlikely that tumors arise in the cornea unless previous vascularization has occurred.6 Spontaneous regression of 30% to 50% of bovine precancerous lesions may occur,1 and in rare cases early OSCC may regress spontaneously. Tumors arising at the limbus are confined by the dense

FIG. 39.19 Bovine ocular squamous cell carcinoma. Note the small mass involving the leading edge of the third eyelid. (Courtesy Dr. JohsH Angelos.)

FIG.
39.20 Bovine ocular squamous cell carcinoma involving the cornea. Note the irregular and invasive growth into the cornea. The surface is rough and necrotic. (Courtesy Dr John Angelos.)and poorly vascularized sclera and cornea, thus hindering metastasis to extraocular sites. Nictitating membrane tumors extend to the base of the membrane and cartilage more rapidly, with spread into the orbit and surrounding bones occurring much sooner than with tumors involving the globe. Although metastasis may eventually occur, extensive extraocular spread
is limited in cattle by the practice of sending most affected animals to slaughter.
■ Epidemiology Although OSCC has been reported in a wide variety of cattle breeds, the Hereford breed (either purebred or crossbred) is most often diagnosed with this tumor as a result of the common use of this breed as a range animal and the strong genetic trait for a white face. Thus selective breeding for partially to fully pigmented periocular skin greatly reduces the occurrence of this tumor.1 The tumor is more common in older cattle, with the peak age prevalence being 7 to 8 years. Exposure to increasing levels of actinic radiation raises the prevalence of bovine OSCC.4 The prevalence of ocular squamous cell tumors, including nonmalignant tumors, involving Hereford herds in regions with abundant sunlight can range from 20% to 40%. Research performed in cattle herds suggests that a high plane of nutrition or a lower-than-normal body weight in cows for the first 2 years acts to increase the prevalence.1 The possibility that bovine OSCC may be induced by viruses (e.g., papillomavirus) warrants further research.
■ Clinical Pathology and Necropsy Findings Definitive diagnosis is achieved by cytologic samples obtained with a spatula after topical anesthesia1 or specimens excised for biopsy and fixed in formalin. Benign lesions typically contain superficial anucleated, keratinized squamous cells and deeper epithelial cells with enlarged nuclei and coarse chromatin clumping.
Biopsies of these lesions show that the basal layer or basement membrane has not been invaded. Malignant OSCC lesions are composed of pleomorphic cells with bizarre shapes, large hyperchromatic nuclei containing large clumps of chromatin, and prominent nucleoli. Invasion across the basement membrane is noted, and keratin-pearl formation or marked anaplasia is usually present.6 In the event of regional lymphatic involvement, fine-needle aspiration or preferably a biopsy may demonstrate neoplastic infiltration.Depending on the extent of tumor invasion, gross changes may be noted that involve the globe, conjunctiva and nictitating membrane, orbit, bones of the orbit, sinuses, and regional lymph nodes. In rare instances, metastasis to thoracic and abdominal organs can occur.
■ Treatment and Prognosis Numerous modalities are available, and applications depend on availability of instrumentation, location and extent of the tumor, and value and intended function of the animal. Choices include radiofrequency hyperthermia (RDM Hypertherm [RDM International, Phoenix, Ariz.]), cryonecrosis, intralesional injection of biologic response modifiers (BRMs) such as allogeneic OSCC extract, mycobacterial cell wall fraction (Normagen [Fort Dodge Laboratories, Fort Dodge, Iowa]), Propionibacterium acnes (ImmunoRegulin [ImmunoVet, Tampa, Fla.]), intralesional chemotherapy with cisplatin (Platinol [Bristol-Meyers, Wallingford, Conn.]) with or without initial debulking,7,8 radiotherapy (cesium-137, cobalt-60, gold-198, iridium, strontium-90), and surgical removal (local excision, enucleation, and exenteration with or without salivary gland and lymph node resection). Intralesional use of cisplatin (1 mg/cm3 of tumor volume) is highly effective, but multiple injections are necessary (four times at 2- to 3-week intervals). Handling of the drug and animal after treatment must adhere to U.S. Occupational Safety and Health Administration (OSHA) guidelines,9 and animals must not be used for food consumption.
Appropriate precautions should be followed with off-label use of cytotoxic drugs. Surgical debulking with adjunctive cryonecrosis or radiofrequency hyperthermia is an effective and affordable treatment modality. Cryonecrosis is achieved with liquid nitrogen, using a probe or spray delivery system to freeze the tissues to -30° C (-22° F) twice, with complete thawing between freeze cycles. Cryotherapy is notrecommended for lesions larger than 0.5 cm in diameter. Massive tissue necrosis and loss of the eyelid can be seen if the lesion is too large.
Radiofrequency hyperthermia is performed with piercing or surface probes to heat the tissues to 50° C (122° F) for 30 seconds.
Because recurrence rates range between 30.4% and 42.4%,3,10 owner compliance to return the animal for follow-up treatment is a significant determinant in overall survival. Financial constraints are the most common reason for cessation of treatment. Many animals that die as a consequence of OSCC are euthanized at the owner's request. The overall prognosis is determined by the degree of neoplastic involvement of normal tissue, but a guarded prognosis is usually warranted. If treatment is undertaken, intervention should begin at the earliest stages of tumor development. In animals destined for slaughter, the guidelines for condemnation of bovine carcasses affected with OSCC shown in part A of Box 39.1 should be considered.
■ Prevention and Control In cattle, factors such as genetics, UV light, and environmental factors (e.g., wind, dust) are known to be involved in OSCC. Ocular viral infection may also be contributory. If possible, affected animals should be culled as soon as possible because most production situations preclude environmental factor modification.
Equine Ocular Squamous Cell Carcinoma
■ Definition and Etiology Equine OSCC is the most prevalent equine ocular neoplasm (followed by equine sarcoid) and typically occurs in horses with nonpigmented eyelids.3,11 Horses with two or more coat colors (Appaloosa, Quarter Horse, Paint) may have minimal ocular and periocular pigmentation. These breeds are at an increased risk of developing equine SCC. Thoroughbreds, Haflingers, and Draft horses (Clydesdale, Belgian, Shire) also have increased prevalence of SCC, even with adequate ocular pigmentation.12 The amount of perilimbal and nictitating membrane pigmentation represents another important causal factor in cattle and horses that has received little attention but should be considered on prepurchase and health examinations (see Chapters 1 and 2).
■ Clinical Signs and Differential Diagnoses Similar tissues are involved in horses as in cattle. These sites include palpebra (eyelids), limbus (corneoscleral junction), conjunctiva, nictitating membrane, and cornea (Color Plate 39.24). Some reports suggest that the nictitating membrane is more frequently involved than the corneoscleral junction.3,11 In addition to the traditional sites, horses also are affected by corneal stromal invasive SCC. The tumor in this location appears as a nonraised mass lesion that grows directly deep into the corneal stroma (see Color Plate 39.13). The smooth appearance may lead to clinical underestimation of the greater underlying tumor invasion.13,14
Differential considerations for OSCC in the horse include adenocarcinoma, adenoma, angiosarcoma, basal cell tumor, conjunctival follicular hyperplasia, dermoid, fibroma, fibrosarcoma, granulation tissue, habronemiasis, lymphosarcoma, mastocytoma, plasma cell tumors, sarcoid, and schwannoma (see Tables 39.4 and 39.5).
■ Pathophysiology Horses demonstrate multiple tumor locations and local invasion in up to 50% of cases.6,10 The tumor has high rates of local infiltration and recurrence.15 Metastasis beyond extraocular sites is rare in horses but has recently been reported in local tissues, such as nasolacrimal duct, regional lymph nodes or maxillary sinus, and more distant sites, such as mediastinum. These metastases occurred without evidence of local recurrence in a delayed fashion, 18 to 42 months following initial therapy.16,17
■ Epidemiology Equine OSCC in North America demonstrates an increased prevalence with increasing longitude (°W), altitude, and mean solar irradiation.11 Breeds with a greater risk of developing OSCC include Draft breeds, especially the Belgian (odds ratio [OR] = 21.7), Appaloosa (Or = 7.9), Paint and Pinto (OR = 4.5), and grade horses (OR = 3.1). Coat colors showing an increased risk include white (OR = 26.7), cremello/palomino (OR = 13.7), gray (OR = 6.7), red/white and strawberry/white (OR = 4.7), buckskin (OR = 4.4), and chestnut/sorrel (OR = 3.8).11 Prevalence increases with age, with the mean age of affected individuals between 9 and 13 years. Bilateral involvement may be as high as 20%.3,10
■ Treatment and Prognosis Surgical excision with adjunctive therapy as described in the Bovine Ocular Squamous Cell Carcinoma section earlier is used in horses. Surgical resection is most effective early in the disease process when clean margins can be obtained. Excision of corneolimbal or corneal SCC via keratectomy followed by adjunctive therapy, such as radiation therapy or cryotherapy, is recommended over surgical excision alone because it is difficult to obtain clean margins in the periocular area.13,15 The most common adjunctive therapies for periocular SCC in horses include cryonecrosis (liquid nitrogen), radiofrequency hyperthermia, intralesional cisplatin or carboplatin, and radiation therapy (cesium-137, cobalt-60, gold-198, strontium-90, iridium).18 Currently the carbon dioxide (CO2) laser is being used for both surgical removal and adjunctive therapy following removal.19 Photodynamic therapy (PDT) can be used alone or in conjunction with surgical removal.20 Recurrence rates were lower following surgical debulking and PDT in comparison to surgical debulking and cryotherapy in a study by Giuliano and colleagues; however, the photosensitizer verteporfin has become increasingly difficult to obtain for veterinary use.20,21 Recurrence rates for ocular and adnexal SCC is high (44.1%). This can be reduced to 11.9% with adjuvant radiation therapy. The anatomic site in horses with the highest recurrence rate was the limbus (corneoscleral junction) or bulbar conjunctiva.14 Medical therapy alone is ineffective as sole treatment for ocular SCC, but it may be an effective adjunctive therapeutic modality. Mitomycin (0.4%) and 1% 5-flourouracil (5-FU) can be used as ophthalmic preparations to treat corneal and eyelid SCC.18,22-24 When applied in an alternating regimen of 7 days on and 7 days off for the cornea, tumor regression was reported for small carcinoma in-situ masses.12
■ Prevention and Control Specific preventive measures have not been systematically evaluated in horses, but recommendations include reducing UV light exposure, using fly masks with UV protection in horses (to decrease solar irradiation and environmental irritants), and avoiding breeds thought to have an increased risk of tumor development. Tattooing of lightly pigmented periocular skin has been performed in hopes of reducing the risk of UV light-induced SCC. This procedure has no deleterious effects, but true efficacy in prevention of SCC is unknown.25
Ovine and Caprine Ocular Squamous Cell Carcinoma
Although rarely reported, SCC of the eye and eyelids has been described in both sheep and goats. Invasive OSCC has been reported in twin goats, but etiology was not elucidated.26 In another study of ovine and caprine cutaneous tumors, ocular tumors (SCC) comprised 11.2% and 13.3% of tumors detected, respectively.27

FIG. 39.21 Orbital lymphosarcoma. Diffuse orbital involvement causing exophthalmos and secondary exposure keratitis of the right eye.
Ocular Manifestations of Lymphosarcoma
■ Definition and Etiology Lymphosarcoma is a fatal systemic neoplastic disease of the lymphoreticular tissue. The adult or enzootic form of bovine lymphosarcoma is likely the most devastating and common neoplasm of dairy cattle. This is a systemic disease with ocular manifestations rather than a primary ophthalmic problem. (See Chapter 37 for specific information regarding bovine lymphosarcoma and the bovine leukemia virus.) Lymphosarcoma represents the most common cause of orbital neoplasia in cattle,28 excluding OSCC that involves the orbit by local extension. Lymphosarcoma may also affect horses29 and goats. The etiology in horses and goats is unknown.
■ Clinical Signs and Differential Diagnoses Clinical signs in cattle are usually associated with exophthalmos caused by orbital invasion of neoplastic lymphoid cells, subsequent exposure keratitis, and eventual proptosis15 (Fig. 39.21). One report documented intraocular lymphosarcoma in a Holstein cow as the presenting sign of generalized lymphosarcoma.30 Subtle exophthalmos is often overlooked because of the natural exophthalmic state of some dairy breeds. Clinical signs associated with the exophthalmos and exposure keratitis include corneal edema, vascularization, ulceration, epidermalization, conjunctival hemorrhage, chemosis, and ocular discharge. These signs may develop, progress, and change quickly once corneal protection is compromised. Other physical examination findings are discussed in Chapter 37. Differential considerations for exophthalmos include orbital cellulitis, trauma, retrobulbar hemorrhage, retrobulbar soft tissue masses, chronic sinusitis, and sinus neoplasia (see Tables 39.4 and 39.5).
Equine lymphosarcoma involving the eye is usually an ocular manifestation of multicentric lymphoma. Other systemic manifestations are discussed in Chapter 37. In one study, ocular lesions were reported in 27% of horses with multicentric lymphoma.31 Ocular manifestations of equine lymphoma include uveitis, nictitating membrane masses, chemosis and conjunctivitis, and neoplastic infiltration of the eyelids and orbit.29,31,32 Several cases of primary ocular lymphoma have also been reported, including one horse with anterior uveitis that was attributed to solitary uveal lymphoma and a horse with corneal lymphoma associated with IMK that had been chronically treated with antiinflammatory medications.33-35 Differential considerations should include conjunctival pseuodotumor36 or follicular conjunctivitis,37 any chronic inflammatory disease, equine infectious anemia, equine piroplasmosis, and infectious causes of uveitis (see Table 39.3).
■ Clinical Pathology and Histopathology Definitive diagnosis of lymphoma is based on cytologic and histopathologic findings. Equine malignant lymphoma is often composed of a heterogenous cell population consisting of B and T lymphocytes.38 Histologic characteristics of lymphoma include compression of normal architecture, a single cell population without organized chromatin pattern, and variable nucleoli size. Tissue samples can also allow for immunophenotyping lymphoma into B- or T- cell origin.39 More information on diagnosing equine lymphoma is available in Chapter 37.
■ Necropsy Findings As with the clinical signs, necropsy findings are variable. In cattle, orbital involvement is common, with lymphoid tumors being firmly attached to the periorbita and walls of the orbit. Extraocular muscles are frequently infiltrated with tumor cells. The globe itself is typically not involved.6 Ocular lesions occur less often in horses than in cattle. In the horse, the globe (uveal tract) can be involved in addition to extraocular tissues. As with other systemic neoplastic diseases, multiple organ involvement is usually expected with lymphoma.
■ Treatment and Prognosis This systemic disease may be treated palliatively or definitively in an attempt to achieve remission for a time. Enucleation provides palliative treatment, and chemotherapy with corticosteroids, vincristine, and L-asparaginase may induce remission. Off-label use of these cytotoxic drugs must be approached with extreme caution, and treated animals must not be used for food consumption. Most cattle with orbital lymphosarcoma either die or are euthanized in terminal stages of disease within 6 months of diagnosis.28,29 Horses can have a much more protracted disease course, with many presenting because of chronic illness of up to 12 months' duration.18 A recent investigation of extraocular lymphosarcoma in 26 horses found that prognosis for remission was fair to good when complete tumor excision could be achieved and there was no eyelid or cutaneous involvement.40 The overall long-term prognosis is unfavorable, regardless of the species involved.
■ Prevention and Control Control of bovine lymphosarcoma depends on efforts to eradicate bovine leukemia virus, a monumental task in most cases. In other large animal species, prevention and control recommendations for lymphosarcoma are not possible until the etiology can be identified. If animals are destined for slaughter, the guidelines for condemnation of bovine carcasses affected with lymphosarcoma as shown in part B of Box 39.1 should be followed.
Ocular Manifestations of Equine Sarcoid
■ Definition and Etiology Equine sarcoid is a locally aggressive, nonmalignant, fibroblastic tumor of equine skin (see Chapter 40). It appears to be the most common equine cutaneous neoplasm, with 14.7% of ocular and adnexal tumors in the horse being sarcoids (all involving the eyelids), making it the second most common eyelid tumor of horses, behind SCC.41 This neoplasm develops more frequently in sites predisposed to trauma and areas that come into contact with existing sarcoids, and it does not metastasize to internal organs. There appears to be a genetically fixed predisposition, which is probably viral induced. Bovine papillomavirus (BPV-1 and BPV-2) DNA was detected in 88% to 100% of sarcoids examined in several studies.42,43 Breed, family, and genetic predispositions have also been identified. Quarter Horses, Appaloosas, and Arabians are at the highest risk, followed by
Thoroughbreds. Standardbreds seem to have the lowest risk.44,45
■ Clinical Signs and Differential Diagnoses Sarcoids involving the eyelids are classified according to the scheme used for cutaneous lesions: verrucous, fibroblastic, mixed, or occult. Tumors of the eyelids may appear smooth and nodular, crusted and nodular, ulcerated, or pedunculated (Figs. 39.22, 39.23, and 39.24). Regardless of their appearance, the tumors are nonregressing. Periocular sarcoids are subject to trauma; thus the verrucous type frequently transforms into the fibroblastic type with surface ulceration. It is difficult to differentiate sarcoid from fibroma, fibrosarcoma, neurofibroma, neurofibrosarcoma, schwannoma, or nonneoplastic granulation tissue (see Tables 39.4 and 39.5).
■ Treatment and Prognosis Problematic tumors can be treated by a variety of modalities, none of which is uniformly successful. Often multiple treatment sessions are required for

FIG. 39.22 Equine sarcoid. Upper eyelid exhibits a smooth nodular mass typical of many periocular sarcoids.
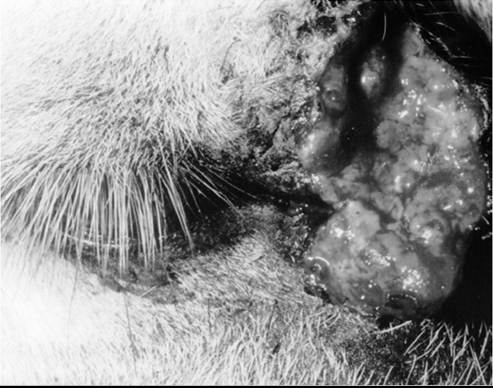
FIG. 39.23 Equine sarcoid involving medial aspect of eyelid. At examination or during treatment, sarcoids may become ulcerated. This tumor became ulcerated after one injection of a Mycobacterium cell wall preparation but subsequently resolved.
tumor control. Treatment modalities that have been reported include surgical excision (50% success rate), cryonecrosis (30% success rate), radiofrequency hyperthermia (RDM Hypertherm), intralesional injection of a BRM (bacille Calmette-Guerin),41 chemotherapy with intralesional cisplatin or carboplatin (with or without initial debulking),6,7 radiation therapy (cesium-137, cobalt-60, gold-198, iridium, strontium-90), and chemotherapy (cisplatin or 5-fluorouracil) combined with surgical excision.46 An available commercial Mycobacterium product (TheraCys®) can be used successfully, but the reported clinical efficacy is variable. If the sarcoid is static, flat, and hairless, it may be best left alone because any trauma—surgical or otherwise—could increase the lesion's growth rate and invasiveness. Topical therapy with the antiviral/anti tumor drug imiquomod (Aldara®) may induce regression in flatter periocular sarcoids, but care should be taken to avoid contact with the conjunctival or corneal surfaces, as the preparation can induce significant ocular irritation.
Intratumoral use of cisplatin is highly effective (see Chapter 40). Response to therapy varies on the basis of tumor location, duration, severity, and previous therapeutic measures.
Although all of these treatment modalities have been used for periocular sarcoids, it is prudent to investigate product availability when developing a treatment plan, as some products vary in their accessibility. Prognosis is favorable for equine periocular sarcoid if a complete treatment protocol is followed. As with any neoplastic disease, at the first evidence of recurrence, the animal should be reevaluated
Miscellaneous Tumors With
Ocular Involvement
The tumors previously discussed represent the most significant ocular or periocular neoplasms of large animals. However, to the individual animal or owner, any tumor type represents a significant problem, even if it is rare. Thus clinicians must remember that numerous primary and secondary neoplastic processes can involve the eye and surrounding tissues. Secondary tumors may be either metastatic masses or locally invasive masses extending from sites near the eye. The greatest variety of ocular neoplastic disease has been reported in the horse (see Table 39.5).
Miscellaneous Adnexal Tumors
Adnexal tumors that have been reported include adenoma, adenocarcinoma, basal cell carcinoma, fibroma, fibrosarcoma,

FIG. 39.24 Multiple equine sarcoids extending from the lateral canthus into periocular tissues.
hemangioma,47 hemangiosarcoma,48 lymphoma, melanocytoma, melanoma,49 papilloma, plasma cell tumors, mast cell tumor,50 hemangiosarcoma,51 and schwannoma. Depending on their location, many of these tumors are amenable to excision and adjunctive therapy, such as cryonecrosis or local chemotherapy.49’5"
Surgical excision of small lesions, cryosurgery, radiation therapy, and intralesional cisplatin7’8 have been the mainstay of treatment for various periocular tumors in the horse. Periocular melanomas have been reported in the horse and are usually seen in older, gray horses (Color Plate 39.24). Most of these masses are benign, and surgical excision is curative, but eyelid reconstructive procedures for larger excisions can be challenging in the horse. A malignant third eyelid melanoma in a gray horse was successfully treated with excision and local chemotherapy.49 Oral use of cimetidine has been reported to shrink dermal melanomas,52’53 but this has not been as successful in other studies,54’55 so is not currently recommended. A recent retrospective study of equine ocular and periocular hemangiosarcomas suggests that early intervention and complete excision yields a good prognosis, whereas in past case reports recurrence was more common and euthanasia of affected horses often resulted. Adjunctive therapies, such as Mitomycin C 0.04% or cryotherapy, were used in most cases in this study.51
Miscellaneous Ocular Tumors Involving the Globe
Reports of neoplasia involving the globe, all in horses, describe the clinical, histologic, and treatment aspects of hemangiosar- coma,51 epibulbar melanocytoma,56 intraocular melanoma,57’58 medulloepithelioma,59 and lymphangiosarcoma.60,61 Intraocular melanomas are rare in horses and are unlikely to metastasize, but secondary glaucoma usually results in enucleation. Ocular melanocytic tumors are more prevalent in horses with a gray coat.58’62’63 Other than vascular tumors, most primary intraocular tumors in horses do not display a severe metastatic threat. Although enucleation may be curative, histologic evaluation of excised tissues and long-term patient follow-up are necessary if accurate epidemiologic and prognostic data are to be available. Once an accurate diagnosis has been made, the clinician and owner must determine, in light of all available medical information and the proposed use of the animal, whether treatment should be curative or palliative or whether elimination of the problem from the herd should be of greater concern than care of the individual animal.
Miscellaneous Orbital Neoplasia
Orbital neoplasia usually present as gradual exophthalmos with or without blindness and mydriasis. Neuroendocrine tumors are the most frequently reported primary orbital tumor in the horse. They rarely metastasize and tend to grow slowly. Exenteration is usually curative, but care must be exercised because there is a large risk for hemorrhage.64’65 Optic nerve tumors include neuroepithelial tumors66 and meningioma.67 An optic nerve neuroepithelial tumor that presented with exophthalmos displayed metastatic spread as a result of extension into the brain through the optic foramen, causing brain compression 2 months after enucleation.66 Other tumors previously documented in the equine orbit include multilobular osteoma (chondroma rodens),68 fibroma,69 angiosarcoma,70 hemangiosarcoma,51 medulloepithe- lioma,71 malignant rhabdoid,72 and adenocarcinoma.65
Any tumor involving the nasal and paranasal cavities has the potential to involve the ocular structures as the result of orbital spread. Enzootic adenocarcinoma in sheep is an example of this type of process. Although infrequently noted, exophthalmos secondary to orbital invasion of this tumor has been reported.73
Central blindness has been reported in a mule with an ependymoma, but could be caused by any type of neoplasia affecting the CNS’ diencephalon’ or occipital cortex.74 Other forms of intracranial neoplasia can secondarily involve the eye as a result of cranial nerve dysfunction. For example’ an intracranial schwannoma caused exposure ulcerative keratitis in a cow that presented with left facial paresis.75
More on the topic Ocular Neoplasia*:
- Ocular Neoplasia*
- Signs of Ocular Disease*
- Ophthalmic History and Examination
- Adnexa
- Horner Syndrome
- Immune-Mediated Ocular Diseases
- Smith Bradford P., Van Metre David C., Pusterla Nicola (eds.). Large Animal Internal Medicine. Part 2. 6th edition. — Elsevier,2020. — 2279 p., 2020
- References
- Lymphoma in Horses
- Smith Mary C., Sherman David M.. Goat Medicine. 3rd edition. — Wiley-Blackwell,2023. — 976 p., 2023