Angular Limb Deformities
Jeffrey P. Watkins
■ Definition, Etiology, and Clinical Signs Angular limb deformities are deviations in the axis of the forelimbs or hindlimbs in the frontal plane. Valgus deformity denotes a lateral deviation of the limb distal to the origin of the deformity; varus deformity denotes a medial deviation.
The deformity is further described by naming the joint adjacent to the origin of the deformity; for example, carpus valgus describes an angular deformity arising in the carpal region, with lateral deviation of the metacarpus (knock-kneed conformation; Fig. 38.1).Angular limb deformities may be either congenital or acquired. In general, they are due to laxity of periarticular supporting structures, incomplete ossification, or asynchronous physeal growth. Potential causes include intrauterine malpo- sitioning, relative immaturity, hereditary predisposition, rapid growth, dietary imbalances, osteochondrosis, and trauma.1-3
Congenital angular deformities are frequently attributed to intrauterine malpositioning and laxity of periarticular supporting structures. They typically originate in the region of the carpus and tarsus, resulting in bilateral valgus deformity. It is also common to identify a “windswept” foal with valgus deformity of one limb accompanied by varus deformity of the contralateral limb. Acquired angular deformities usually occur secondary to asynchronous growth. In addition, a foal born with incomplete ossification may acquire an angular deformity secondary to crushing of the cartilaginous precursors of the cuboidal bones. A hereditary angular limb deformity of Suffolk, Suffolk crossbred, and Hampshire sheep is known as spider lamb syndrome (see the Ovine Hereditary Chondrodysplasia [Spider Lamb Syndrome] section later).
■ Pathophysiology Incomplete ossification is an important cause of angular deformities originating at the carpus and tarsus.
The epiphyses and cuboidal bones of the carpus (ulnar, third, and fourth carpal bones) and tarsus (central and third tarsal bones) are primarily affected.1 Most ossification of the cartilaginous precursors of these bones occurs in late gestation and is complete by the first month after birth. Prematurity or relative immaturity results in the birth of a foal before these precursors are completely ossified (Figs. 38.2 and 38.3). If laxity of the periarticular supporting structures accompanies incomplete ossification, the deformity is congenital and may worsen progressively with weight bearing as the cartilaginous cuboidal bone precursors become deformed. If laxity is not present, the foal may be born with straight legs and with unrestricted exercise acquire an angular deformity due to deformation of the precursors of the cuboidal bones during weight-bearing activity. Foals that acquire significant deformation of the developing cuboidal bones are likely to develop osteoarthritis early in life and have limited ability to perform athletically as adults.Foals can acquire an angular limb deformity because of asynchronous growth at the metaphyseal and epiphyseal growth cartilages.2,3 An important cause of asynchronous growth is trauma to a portion of the growth cartilage of the physis.4 In many foals this trauma is in the form of nonphysiologic compression of the growth cartilage. Excessive exercise in foals
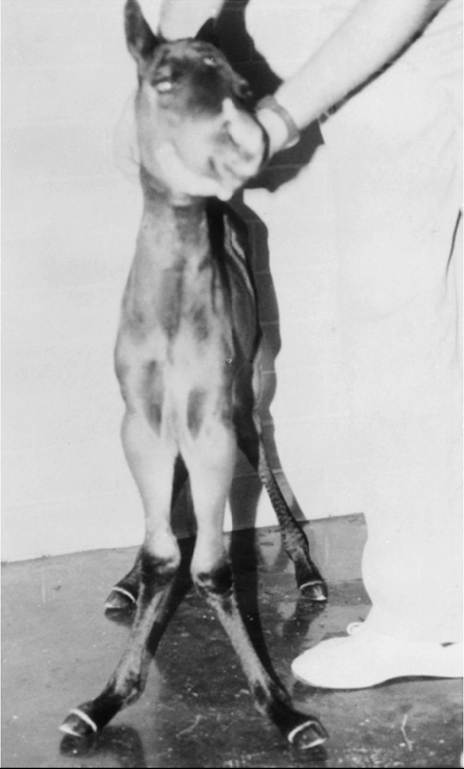
FIG. 38.2 Premature foal with incomplete ossification of the cuboidal carpal bones, showing marked bilateral carpus valgus.
with mild angulation and normal activity in foals with moderate to severe preexisting angular deformity may result in sufficient trauma to the growth cartilage to cause progressive deformity.
Asymmetric loading also occurs when severe lameness is present. With the change from a rectangular stance with four weight-bearing limbs to a triangular stance with three weightbearing limbs, asymmetric, nonphysiologic loading of the contralateral support limb occurs, which predisposes it to developing an angular deformity.
Chronic excessive loading stretches the periarticular ligamentous support on the lateral aspect of the limb. Combined with compressive forces that are concentrated along the medial aspect of the growth cartilages negatively affecting normal growth at the physis, a varus deformity often develops in the overloaded support limb.Abnormalities of the growth cartilage that affect ossification (e.g., osteochondrosis) may also be responsible for angular deformities caused by asynchronous growth. Foals with a predisposition for rapid growth or those exposed to nutritional imbalances appear to be at greatest risk for developing the disease. Rapid growth may also result in a foal with a large body size disproportionate to its skeletal structures. This condition may cause increased compressive forces, nonphysiologic loading of the growth cartilages, and angular deformity.4 Rarely, hypothyroidism in foals, either due to maternal influences related to excessive or inadequate dietary iodine or due to plant toxicity, has been related to delayed ossification of the cuboidal bones.5 In addition, in the northwestern United States and adjacent area or Canada, hypothyroidism of undetermined cause in foals has been associated with skeletal abnormalities.6
Ruminants raised in confinement may experience endochondral dysplasia and angular limb deformities if dietary iron

FIG. 38.3 Specimen from a foreleg of the premature foal in Fig. 38.2, cut in the frontal plane. Note the thick cartilage surrounding the centers of ossification of the cuboidal bones of the carpus.
is high or dietary vitamin D is low7 (rickets). Elevated dietary iron results in elevations in serum phosphorus, which in turn may inhibit 1,25-dihydroxycholecalciferol synthesis by the kidney, resulting in rickets.5 Pregnancy-associated epiphysitis in primiparous dairy goats8 can also result in angular limb deformities.
■ Evaluation and Radiographic Findings When evaluating a foal with an angular deformity, important historical information includes gestational length, age of the foal, onset and progression of the deformity, and intended use of the foal. The foal should be observed carefully while standing and walking to characterize the degree of deformity and determine the presence of compensatory problems or lameness. Physical examination includes careful palpation of the affected limb and, in neonates, determination of whether the deformity can be corrected by manual manipulation of the limb and whether there is evidence of prematurity or dysmaturity. In neonates, deformities resulting from laxity of periarticular supporting structures and incomplete ossification can often be corrected manually. In older foals, if deformities secondary to incomplete ossification have been left untreated and the cuboidal bones are in a collapsed configuration, or if deformities are the result of asynchronous growth, the angulation in the limb cannot be corrected manually.
Visual assessment of the forelimbs and hindlimbs from all angles is necessary, making note of the relative angulation through each joint in the sagittal plane of the evaluated limb. It should be noted that the degree of external rotation of the limb being inspected determines the position where the examiner should make his or her evaluation. In most cases external rotation is present in the limb, which necessitates examining each limb independently from a position that is slightly oblique to the median axis of the body (cranial to caudal, lateral to medial). A normal foal should have alignment of the third metabone with the phalanges, and any deviation should be considered abnormal. There is normally a mild valgus deformity in foals through the carpus and tarsus, which at weaning is in the vicinity of 5 degrees, that usually resolves as they approach their yearling year. In addition to evaluating the angulation of the hindlimb in the sagittal plane, it is important to assess hock angulation in the frontal plane.
Sickle-hock conformation can be the result of incomplete ossification with collapse of the central and/or third tarsal bones.An arthropathy should be suspected if lameness is present. A reduced range of motion and pain on passive flexion of affected joints may also be present. Collapse of incompletely ossified cuboidal bones may cause deformation of articular surfaces resulting in DJD and be manifest by the above findings. When this occurs in the carpus, the prognosis for athletic performance is guarded to poor. If the cuboidal bones of the tarsus are affected, mild collapse may not adversely affect performance, but with significant collapse, degenerative change is likely. A less common cause of lameness in foals with angular limb deformity is osteochondrosis. The prognosis for athletic performance in foals with osteochondrosis-associated angular limb deformities depends on the severity of the osteochondral lesions.
Radiographic evaluation of foals with angular deformity is important. If a diagnosis of incomplete ossification is delayed, irreparable damage may occur. In fact, a strong argument can be made for radiographic evaluation of all foals shortly after birth before uncontrolled exercise is allowed. Radiographic evaluation is mandatory to determine the degree of ossification in premature foals, twins, foals that appear to be relatively immature at birth, and foals born with angular deformities.
In addition to assessing the maturity of the cuboidal bones, radiographic evaluation allows the examiner to identify the origin of the deformity and determine its severity. Dorsopalmar views for the carpus and fetlock and a lateromedial view of
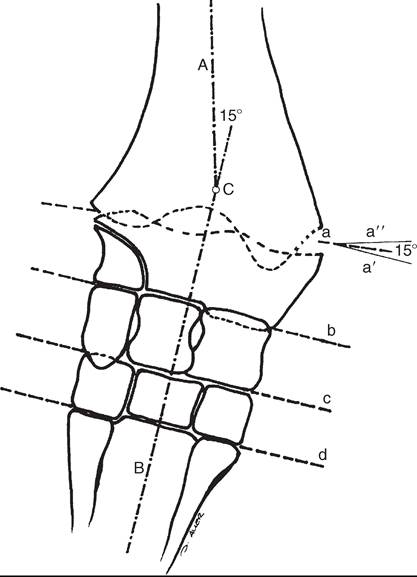
FIG. 38.4 Two methods for geometric evaluation of an angular deformity at the carpus. Lines A and B are drawn through the long axis of the radius and metacarpus, respectively. The angle of incidence is 15 degrees. Lines a, b, c, and d are drawn through the distal radius physis, antebrachiocarpal (radiocarpal), middle, and carpometacarpal joints, respectively.
Line a, is drawn parallel to line b, and line a" is perpendicular to A. Their angle of incidence is 15 degrees. (Reprinted with permission from Compend Contin Educ Pract Vet 4:S330, 1982.)the tarsus are recommended. In the carpus and fetlock, the origin of the deformity may be subjectively determined by two geometric methods (Fig. 38.4). One method is to draw longitudinal lines bisecting the long bones above and below the joint. Where these lines intersect is the pivot point, which is considered the origin of the deformity; the angle of incidence of these lines is an estimation of the degree of deformity. Another method is to draw lines through the joints and adjacent physes. These lines should be parallel to each other and perpendicular to the long axis of the long bones proximal and distal to the affected joint. The origin and degree of deformity are estimated by determining where and by what degree these lines deviate from normal. Both asynchronous growth and incomplete ossification can occur concurrently, which is most easily determined with the latter method of geometric evalu- ation1 (Fig. 38.5). Geometric examination to determine the degree of deformity in the tarsus is less reliable because the tibia and third metatarsus are not in the same frontal plane. The severity of the angular deformity in this location is best determined by a careful visual assessment.
Radiographic findings in foals with incomplete ossification vary depending on the degree of mineralization of the precursor cuboid bones and amount of malformation that has occurred subsequent to birth. In severe cases, there may be only small, centrally located centers of ossification surrounded by radiolucent precursor cartilage (which will undergo endochondral ossification as maturity progresses). More commonly, affected cuboidal bones have a rounded contour instead of their normal angular appearance. The width of the radiolucent precursor cartilage is increased, appearing radiographically as an increase
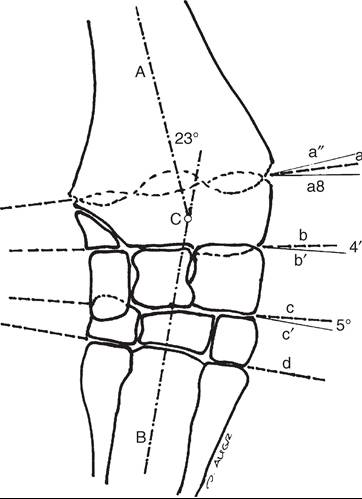
FIG. 38.5 Geometric evaluation of an angular deformity at the carpus caused by a combination of asynchronous growth and incomplete ossification. The pivot point, C, identified by lines A and B, indicates that the origin of the deformity is in the distal radial physis. However, lines a, b, c, and d are not parallel to each other, and lines a, b, and c are not perpendicular to the long axis of the metacarpus and radius. Their orientation indicates that the deformity is in the distal radial physis and the cuboidal bones as well. Note that the sum of angles a-a,, b-b,, and c-c, equals the angle of incidence of lines A and B. (Reprinted with permission from Compend Contin Educ Pract Vet 4:S330, 1982.)
in the width of the joint space (Fig. 38.6). As ossification progresses, the bones may develop a normal anatomic shape or appear wedge shaped or crushed because of deformation of the cartilage secondary to weight bearing prior to ossifying. This phenomenon often is noted in the ulnar, fourth, and intermediate facet of the third carpal bones in the forelimb and the central and third tarsal bones in the hindlimb. In severe cases the affected bones may be grossly deformed and, particularly in the tarsus, appear to be partially extruded from the joint (Fig. 38.7). In the tarsus, lateromedial radiographs are used to determine whether ossification is complete and malformation is present (Fig. 38.8).
Radiographic evaluation of foals with angular deformity caused by asynchronous growth may show wedging of the epiphysis (Fig. 38.9), widening of the physis, and sclerosis adjacent to the physis. Geometric evaluation places the deviation in the metaphysis or the epiphysis of the long bone proximal to the affected joint. The joints are parallel to each other and perpendicular to the longitudinal axis of the adjacent long bones.
■ Treatment and Prognosis Neonatal foals with an angular deformity should be confined to a stall until clinical and radiographic examinations are completed. If the deformity is 10 degrees or less and radiographs reveal normal ossification, stall confinement with periods of controlled exercise is recommended. This regimen promotes continued development of the supporting structures while minimizing trauma to growth cartilages that could result if the foal were allowed uncontrolled exercise. Foals that have angular deformity severe enough to cause the hoof to break over the lateral (varus deformity) or medial (valgus deformity) wall will benefit from the application of a hoof plate. The hoof plate is intended to extend the solar

FIG. 38.6 Dorsopalmar radiograph of a foal with mild incomplete ossification of the cuboidal carpal bones. Note the difference in width of the medial aspect (a) and the lateral aspect (b) of the third carpal bone. Normally, width a should be approximately three-fourths the width of b. Also note the appearance of an increase in the width of the joint space (c) as a result of incompletely ossified joint cartilage.
surface of the hoof to counteract the forces resulting in the abnormal breakover.
Foals with a congenital angular deformity of more than 10 degrees that can be manually corrected should be considered candidates for external support, especially if incomplete ossification is present. Patients with incomplete ossification accompanied by angular deformity that is not supported in axial alignment will often deform the cartilaginous cuboidal bone precursors with continued weight bearing. Subsequent ossification results in permanent deformity of the affected bones (see Fig. 38.7) and is often associated with end-stage osteoarthritis.
Methods of externally supporting the carpus and tarsus vary from tube casts or rigid splints to custom-made orthotic devices. Tube casts have been recommended and used successfully,1-3 and although they provide the rigid external support necessary to maintain axial alignment while ossification progresses, several potential complications are associated with their use. The most serious is the potential for coxofemoral luxation when tube casts are used on the hindlimbs. In addition, foal skin is easily

FIG. 38.7 Dorsopalmar radiograph of a foal with incomplete ossification that was not externally supported. Severe deformation and collapse of the fourth and third carpal and proximal fourth metacarpal bones have occurred.
traumatized by a poorly fitting cast, and deep ulcerations may occur. Other considerations include the cost of materials and the need for constant monitoring to detect signs of a poorly fitting cast. Monitoring the status of a cast requires daily evaluation by a trained individual, and owners are seldom capable or willing to take on this responsibility; hospitalization is recommended. Rigid splints, usually fashioned from cut sections of polyvinyl chloride (PVC) pipe, are an alternative method of support. The leg is protected with a well-padded support bandage, and the splint is applied with nonelastic tape while the limb is held in alignment by an assistant. These splint bandages are changed frequently, as pressure sores beneath the splint bandage are a concern and are difficult to prevent. A splint for the tarsus may be fashioned from synthetic casting material molded lengthwise over the cranial aspect of a padded bandage centered at the joint. Once the material has dried, the splint is taped to the dorsal surface of the bandage. Alternatively, a PVC splint can be heated and bent to the desired angulation.
Regardless of the means of external support used for the carpus or tarsus, it should not extend beyond the distal metabone. Continued weight bearing by the suspensory apparatus of the fetlock helps prevent the development of fetlock hyperextension after removal of the external support. A degree of carpal hyperextension is usually present immediately after removal of external support from the forelimb, and exercise

FIG. 38.8 Lateromedial radiograph of a tarsus from a foal with incomplete ossification. Note the lack of an angular appearance of the central tarsal bone and incomplete ossification of the third tarsal bone.
should be controlled until the tendons and periarticular supporting structures regain their normal tone.
Foals with an angular deformity resulting from asynchronous growth should have their exercise limited to minimize the magnitude of asymmetric loading at the growth cartilages and to encourage spontaneous correction. In these cases, reducing the magnitude of the forces acting asymmetrically at the growth cartilage should encourage compensatory growth to occur and correct the deformity. Additional therapy consists of corrective hoof trimming. Because foals with valgus deformity typically have a toe-out conformation, emphasis in the past has been to lower the lateral hoof wall of the affected limb. If this mode of therapy is vigorously pursued, compensatory varus deformity may develop in the fetlock region. This form of corrective trimming concentrates forces asymmetrically on the medial aspect of the distal metacarpal and proximal phalangeal growth cartilages. Currently, trimming the hoof level and squaring the toe to promote breakover at the toe are recommended.
Foals with angular limb deformities that fail to respond to conservative methods are candidates for surgical intervention. Animals with angular deformities arising distal to the physis were not considered candidates for surgical therapy in the past, but it has been shown that they can respond favorably to surgery.9,10
The decision for surgery should consider the area affected (fetlock, carpus, and/or tarsus) amount of correction required (degree of deformity), and age of the foal. In general, the more severe the deformity, the earlier the surgical intervention should be. Timing of surgery should consider the periods of rapid and predictable growth at the physis. The most rapid and

FIG. 38.9 Dorsopalmar radiograph of a foal with angular deformity caused by wedging in the distal radial epiphysis, the result of asynchronous growth of the epiphysis growth cartilage.
predictable rate of growth occurs from birth to 10 weeks of age.11 In the distal radius, continuous but declining growth occurs until 60 weeks of age. In the distal third metacarpal and metatarsal bones, growth rate slows dramatically by 10 weeks of age and is minimal thereafter. For these reasons, it is important to be more proactive and intervene at an early age when deformities are present in the fetlock region since there is limited time for conservative therapy to effect correction. However, there is more opportunity for correction to occur spontaneously in the carpal and tarsal region; therefore surgical intervention can be delayed in mild to moderate deformities.
Surgical manipulation of physeal growth is intended to asymmetrically alter the elongation occurring at the physis, thereby realigning the axis of the limb. Growth at the physis can be altered surgically in one of two ways: retardation or acceleration. Growth retardation is accomplished by bridging the physis with metallic implants. When applied to the convex side of the affected physis, growth is disallowed on the long side of the bone while continued growth on the opposite side of the bone brings the limb into alignment. As long as the implants are in place, the effect continues and is limited only by the amount of growth remaining at the physis. If the physis is still active once the limb is aligned, it is extremely important that the implants be removed, or overcorrection will occur. Techniques of transphyseal bridging include stapling, screw and wire implants, use of a small bone plate, and more recently a single transphyseal screw. Indications for transphyseal bridging include deformities that have a limited window of opportunity to correct (e.g., moderate to severe deformity in the fetlock region), those presenting after the period of rapid and reliable physeal growth, severe angulations, and based on the author's experience, deformities of the carpus and tarsus resulting from cuboidal bone malformations.
The second surgical approach to altering physeal growth, periosteal transection and elevation (stripping), is intended to accelerate growth on the concave side of the bone.12 Reported advantages include rapid correction without the potential for overcorrection.9,12 Because periosteal transection does not require implants, the likelihood of infection and excessive fibrosis is reduced. Implant failure is not a consideration, and a second surgery for implant removal is unnecessary. The procedure does not require specialized equipment and is technically easy to perform. In one series of foals, correction of the deformity occurred in 22 of 25 limbs treated with periosteal transection.12 In a second series of 23 foals, 83% had straight limbs and were sound for their intended use at long-term follow-up. The success rate was not affected by the origin of the deformity, degree of deviation, or presence of mild to moderate morphologic changes in the involved bones.12 There are reports that question the efficacy of this procedure, particularly for treating carpus valgus deformities.13,14
Indications include mild to moderate deformities present during the rapid, reliable growth at the involved physis. Furthermore, it should be reserved for deformities in locations that will allow ample time for a second procedure to be performed if the initial treatment is not effective. The periosteum will reestablish itself, so the surgical effect is short-lived, and if correction is not adequate within 4 to 6 weeks, additional therapy is indicated.
More on the topic Angular Limb Deformities:
- Angular Limb Deformities
- Physitis (Epiphysitis)
- Postural Deformities
- REFERENCES
- Sprains, Subluxations, and Luxations
- Osteoarthritis
- Septic Arthritis and Osteomyelitis
- Fractures
- Hands-on Examination
- Septic (Infectious) Arthritis and Osteomyelitis